The benefit of omega-3 supplementation has been debated in the cardiology and nutritional literature for many years. Most studies of supplementation have failed to measure tissue levels achieved and often used very low doses. But when tissue levels were measured, either in the serum or red blood cell membrane, the studies consistently demonstrated significant reductions in all-cause mortality and cardiovascular mortality associated with high levels of omega-3 fatty acids.
In addition, higher levels of omega 3 are associated with >=80% reduction in sudden death associated with acute myocardial infarction (acute MI) and > 80% reduction in sudden death in cohorts without known coronary artery disease followed long term.
Two Coronary CT Angiogram (CCTA) studies demonstrated that patients with stable coronary artery disease on statin therapy randomized to high dose EPA and DHA had “prevention of coronary plaque progression when an omega-3 fatty acid index >= 4% was achieved.”
Another CCTA study demonstrated that patients receiving omega 3 supplementation had significantly less coronary atherosclerotic “high risk” lipid rich plaque prevalence (3.8% versus 32%) and lower total non-calcified plaque burden independent of cardiovascular risk factors compared to matched controls not receiving omega 3 supplements.
Omega 3 supplementation after an acute myocardial infarction has been found to reduce infarct size, reduce scaring (fibrosis), and enhance heart tissue healing. (Randomized controlled clinical trial) However a post MI study in 1027 elderly patients randomized to receive 1.8 grams per day of EPA+DHA versus a control group receiving corn oil showed no reduction in the primary composite cardiovascular endpoint between the two groups at 2 years but a higher incidence of AF in the omega 3 group that did not reach statistical significance.
Recently a study, widely reported by the lay press, suggested that high dose omega-3 supplementation was associated with increased risk of atrial fibrillation (AF). These results conflicted with previous studies which demonstrated just the opposite, specifically prior studies demonstrated reduced risk of AF. The more recent study suffered a significant design flaw. The study in question failed to make statistical adjustment for the increased life span associated with higher levels of omega-3. Since age is a primary risk factor for AF, any intervention which increases life span would be expected to result in more AF over the lifetime of the patients as they aged (i.e., more elder years results in increased risk of AF). Therefore, statistical adjustment for that effect should be employed, but was not done in the study.
Unfortunately, science journalism has deteriorated to a state where the conclusions of study authors are most often quoted without interpretation or context, and without critical analysis or comparisons with previous studies that may have demonstrated opposing results.
In addition to large well-designed studies that have suggested a reduced risk of AF associated with omega-3 fatty acids, there have been natural experiments that provide reassuring information. The indigenous Inuit people of Greenland, for example, historically consumed large amounts of omega-3 in their diet with no evidence of increased risk of AF. In fact, before the introduction of western processed foods, estimates of AF among the Inuit were 0.6% (1963) compared to a “worldwide prevalence of AF in adults between 2 and 4%, between one and two percent in Canadian and the general US population and between 0.5% and 3% in most low- and middle-income countries.” A more recent study of Greenland yielded a prevalence of 1.4% likely reflecting a change in habits consisting of less exercise, more tobacco use and a shift to a more Western diet.
Still, multiple studies that used high dose omega 3 supplements in patients with known cardiac disease suggest an increased risk of AF. A good review of omega-3 fatty acids and atrial fibrillation was published in the Korean Journal of Internal Medicine, referenced below.
My interpretation of the complex data in this area is as follows.
At supplemental doses of EPA+DHA above 1.8 grams per day (and perhaps above 1 gram per day) in patients with known coronary artery disease (CAD), at high risk of CAD, or following a myocardial infarction, the risk of AF is increased by about 25% (relative risk). But the risk of lethal ventricular arrythmias (sudden death) associated with myocardial infarction (heart attack) is 80% lower in patients with a red blood cell omega 3 index of >=8. In people without known CAD, an omega-3 index >=8% is associated with an 80% reduction in sudden cardiac death. CCTA studies show significantly lower unstable “vulnerable” plaque in patients on omega-3 supplements. Similarly, omega 3 supplementation in patients on statins associates with halted plaque progression determined by serial CCTA in non-diabetics.
In addition, higher tissue levels of omega 3 are associated with significantly reduced all-cause, cardiovascular, and cancer mortality.
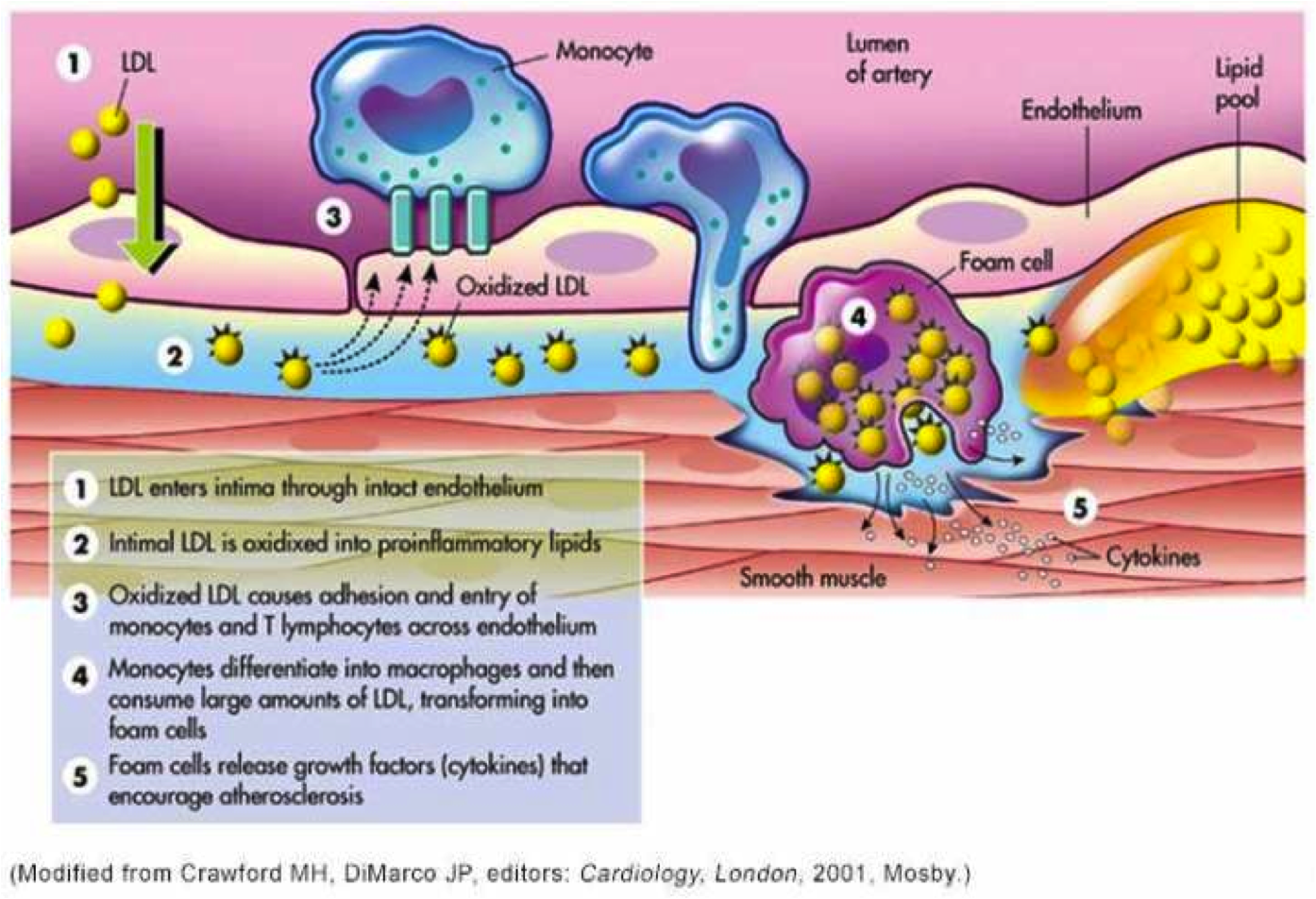
Omega-3 fatty acids are the chemical precursors of SPMs, specialized pro-resolving lipid mediators which help resolve inflammation. We know that cardiovascular events are driven by chronic inflammation in the walls of arteries, often mediated by insulin resistance. Chronic inflammation contributes to atherosclerosis (production of plaque in the artery wall) as well as cardiovascular events that result when unstable plaque ruptures. Studies suggest that n-3 fatty acids may have antiarrhythmic properties with membrane-stabilizing effects in addition to antithrombotic and anti-inflammatory properties on the endothelial level. Basic science, observational studies and clinical trials have demonstrated that higher tissue levels of omega 3 fatty acids are associated with longer health span and lifespan. This understanding must be balanced with a probable increased risk of AF in certain clinical situations associated with high dose omega-3 supplements as described above (people with known CAD, high risk for CAD, or following and MI). Note that current AHA and ACC dietary guidelines include at least 2 servings of fatty fish per week, one serving provides approximately 1800 mg of omega-3.
Getting omega-3 fatty acids from cold water fatty fish would be ideal. Unfortunately, many individuals do not like salmon, sardines, mackerel or herring and simply will not consume enough of this fish to achieve protective tissue levels. Other species of fish and seafood provide much less amounts of omega 3. Another consideration is that individuals process omega 3 fats differently so different amounts of omega 3 will be necessary to reach the same protective levels in tissue. You can obtain a red blood cell omega-3 index using a home kit and a finger prick without a prescription (https://omegaquant.com/). The sample is mailed in to the lab and results reported directly to you. I have no financial relationship with these folks.
Bill Harris, PhD, is widely published in the area of omega-3 science. He developed the first clinically useful tissue assay which measures the % of omega 3 fat in red blood cell membranes, the “omega-3 index” which is the gold standard for omega 3 research and clinical testing. Although serum levels correlate with the red blood cell index, the later reveals dietary consequences of a 2-3 month period while serum levels reflect just a few days of most recent dietary habits. The red blood cell omega 3 index is analogous to the hemoglobin A1c which reveals average blood sugars over a 2–3-month period. Bill Harris suggests that 1800 mg per day of omega 3 fat consumption (food plus supplements) will achieve an index of >= 8% in most individuals.
Here are some references.
Harris WS, Tintle NL et.al., Fatty Acids and Outcomes Research Consortium (FORCE). Blood n-3 fatty acid levels and total and cause-specific mortality from 17 prospective studies. Nat Communications. 2021 Apr 22;12(1):2329. doi: 10.1038/s41467-021-22370-2. PMID: 33888689; PMCID: PMC8062567. https://pubmed.ncbi.nlm.nih.gov/33888689/
“Here we report the results of a de novo pooled analysis conducted with data from 17 prospective cohort studies examining the associations between blood omega-3 fatty acid levels and risk for all-cause mortality. Over a median of 16 years of follow-up, 15,720 deaths occurred among 42,466 individuals. We found that, after multivariable adjustment for relevant risk factors, risk for death from all causes was significantly lower (by 15-18%, at least p < 0.003) in the highest vs the lowest quintile for circulating long chain (20-22 carbon) omega-3 fatty acids (eicosapentaenoic, docosapentaenoic, and docosahexaenoic acids). Similar relationships were seen for death from cardiovascular disease, cancer and other causes”
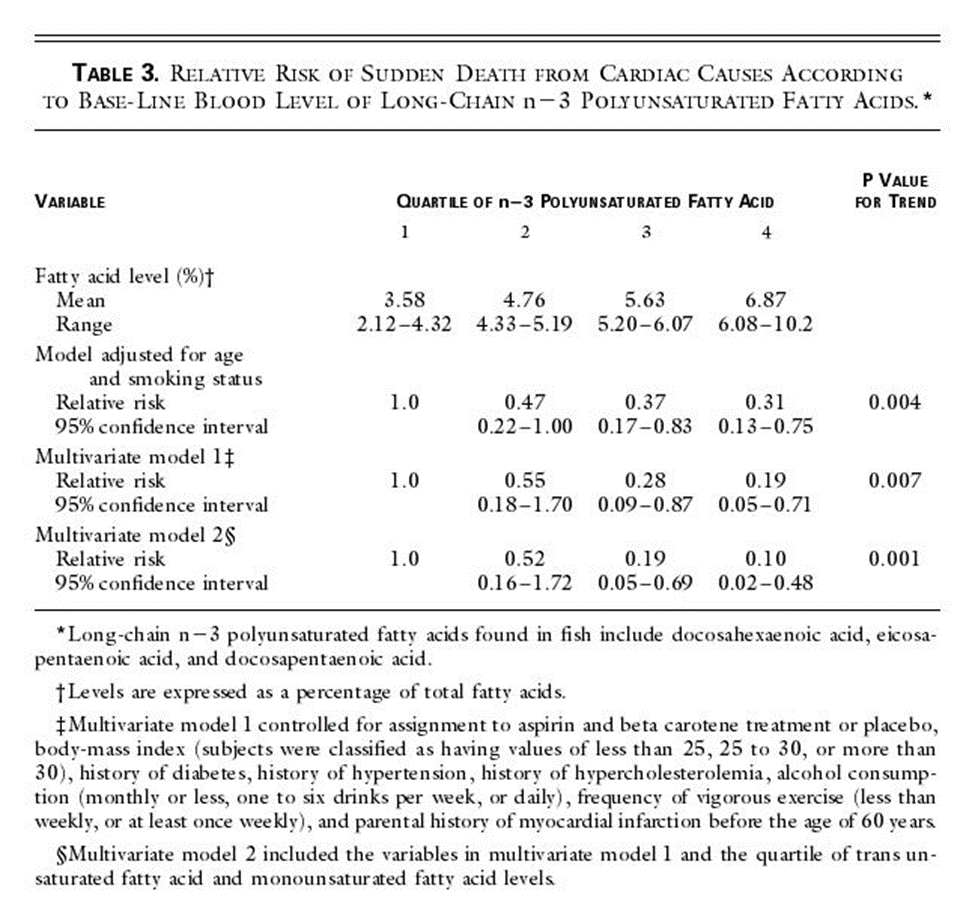
Blood Levels of Long-Chain n–3 Fatty Acids and the Risk of Sudden Death Authors: Christine M. Albert, M.D., M.P.H., Hannia Campos, Ph.D., Meir J. Stampfer, M.D., Dr.P.H., Paul M. Ridker, M.D., M.P.H., JoAnn E. Manson, M.D., Dr.P.H., Walter C. Willett, M.D., Dr.P.H., and Jing Ma, M.D., Ph.D.
Published April 11, 2002 N Engl J Med 2002;346:1113-1118DOI:10.1056/NEJMoa012918 VOL. 346 NO. 15 https://www.nejm.org/doi/full/10.1056/NEJMoa012918
We conducted a prospective, nested case–control analysis among apparently healthy men who were followed for up to 17 years in the Physicians’ Health Study. The fatty-acid composition of previously collected blood was analyzed by gas–liquid chromatography for 94 men in whom sudden death occurred as the first manifestation of cardiovascular disease and for 184 controls matched with them for age and smoking status.
RESULTS
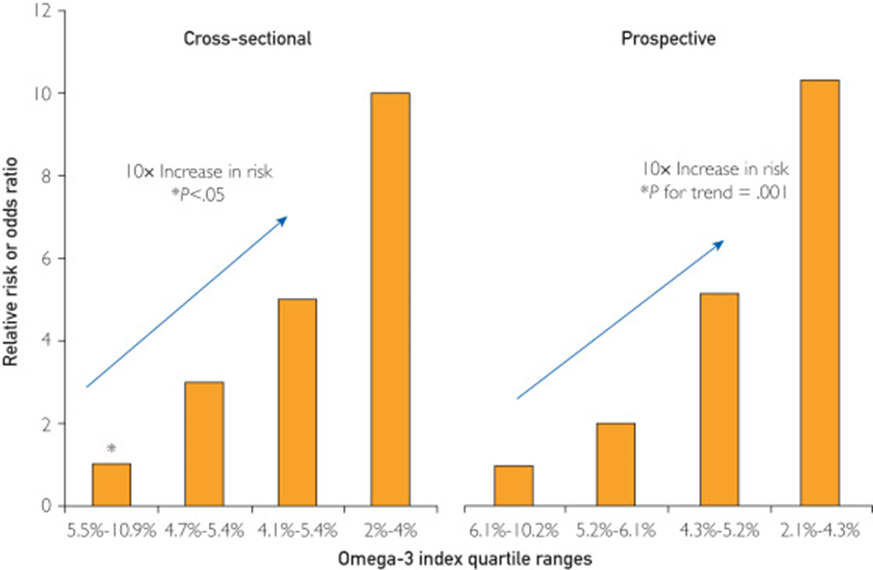
Base-line blood levels of long-chain n–3 fatty acids were inversely related to the risk of sudden death both before adjustment for potential confounders (P for trend = 0.004) and after such adjustment (P for trend = 0.007). As compared with men whose blood levels of long-chain n–3 fatty acids were in the lowest quartile, the relative risk of sudden death was significantly lower among men with levels in the third quartile (adjusted relative risk, 0.28; 95 percent confidence interval, 0.09 to 0.87) and the fourth quartile (adjusted relative risk, 0.19; 95 percent confidence interval, 0.05 to 0.71).
CONCLUSIONS
The n–3 fatty acids found in fish are strongly associated with a reduced risk of sudden death among men without evidence of prior cardiovascular disease.
Heydari B, Abdullah S, Pottala JV, Shah R, Abbasi S, Mandry D, Francis SA, Lumish H, Ghoshhajra BB, Hoffmann U, Appelbaum E, Feng JH, Blankstein R, Steigner M, McConnell JP, Harris W, Antman EM, Jerosch-Herold M, Kwong RY. Effect of Omega-3 Acid Ethyl Esters on Left Ventricular Remodeling After Acute Myocardial Infarction: The OMEGA-REMODEL Randomized Clinical Trial. Circulation. 2016 Aug 2;134(5):378-91. doi: 10.1161/CIRCULATIONAHA.115.019949. PMID: 27482002; PMCID: PMC4973577. https://www.ahajournals.org/doi/10.1161/CIRCULATIONAHA.115.019949
Conclusions: Treatment of patients with acute myocardial infarction with high-dose omega-3 fatty acids was associated with reduction of adverse left ventricular remodeling, noninfarct myocardial fibrosis, and serum biomarkers of systemic inflammation beyond current guideline-based standard of care.
Effect of Different Antilipidemic Agents and Diets on Mortality A Systematic Review
Studer M, Briel M, Leimenstoll B, Glass TR, Bucher HC. Effect of Different Antilipidemic Agents and Diets on Mortality: A Systematic Review. Arch Intern Med. 2005;165(7):725–730. doi:10.1001/archinte.165.7.725
Compared with control groups, risk ratios for cardiac mortality indicated benefit from statins (0.78; 95% CI, 0.72-0.84), resins (0.70; 95% CI, 0.50-0.99) and n-3 fatty acids (0.68; 95% CI, 0.52-0.90).
Feuchtner G, Langer C, Barbieri F, Beyer C, Dichtl W, Friedrich G, Schgoer W, Widmann G, Plank F. The effect of omega-3 fatty acids on coronary atherosclerosis quantified by coronary computed tomography angiography. Clin Nutr. 2021 Mar;40(3):1123-1129. doi: 10.1016/j.clnu.2020.07.016. Epub 2020 Jul 22. PMID: 32778459. https://pubmed.ncbi.nlm.nih.gov/32778459/
Conclusions: Omega-3-PUFA supplementation is associated with less coronary atherosclerotic “high-risk” plaque (lipid-rich) and lower total non-calcified plaque burden independent on cardiovascular risk factors. Our study supports direct anti-atherogenic effects of Omega-3-PUFA.
Alfaddagh A, Elajami TK, Saleh M, Mohebali D, Bistrian BR, Welty FK. An omega-3 fatty acid plasma index ≥4% prevents progression of coronary artery plaque in patients with coronary artery disease on statin treatment. Atherosclerosis. 2019 Jun;285:153-162. doi: 10.1016/j.atherosclerosis.2019.04.213. Epub 2019 Apr 13. PMID: 31055222; PMCID: PMC7963401.An omega-3 fatty acid plasma index ≥4% prevents progression of coronary artery plaque in patients with coronary artery disease on statin treatment – PMC (nih.gov)
Conclusions: EPA and DHA added to statins prevented coronary plaque progression in nondiabetic subjects with mean LDL-C <80 mg/dL, when an omega-3 index ≥4% was achieved. Low omega-3 index <3.43% identified nondiabetic subjects at risk of coronary plaque progression despite statin therapy
Association of Plasma Phospholipid Long-Chain Omega-3 FattyAcids with Incident Atrial Fibrillation in Older Adults: The Cardiovascular Health Study, Circulation Volume 125, Number 9 https://doi.org/10.1161/CIRCULATIONAHA.111.062653
Among 3326 US men and women ≥65 years of age and free of AF or heart failure at baseline, plasma phospholipid levels of eicosapentaenoic acid, docosapentaenoic acid, and docosahexaenoic acid were measured at baseline by use of standardized methods. Incident AF (789 cases) was identified prospectively from hospital discharge records and study visit ECGs during 31 169 person-years of follow-up (1992-2006).
Conclusions: In older adults, higher circulating total long-chain n-3 PUFA and docosahexaenoic acid levels were associated with lower risk of incident AF (atrial fibrillation). These results highlight the need to evaluate whether increased dietary intake of these fatty acids could be effective for the primary prevention of AF.
Omega-3 Fatty Acid Therapy: The Tide Turns for a Fish Story https://www.mayoclinicproceedings.org/article/S0025-6196(16)30764-9/fulltext
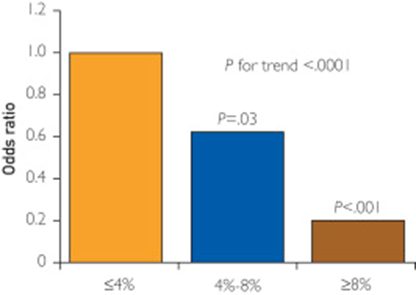
An omega-3 index of less than 4% is associated with increased CHD risk, particularly for sudden cardiac death. In contrast, an omega-3 index of more than 8% is associated with low CHD risk, whereas the range between 4% and 8% is considered intermediate risk
Risk of sudden death
Alfaddagh A, Elajami TK, Ashfaque H, Saleh M, Bistrian BR, Welty FK. Effect of Eicosapentaenoic and Docosahexaenoic Acids Added to Statin Therapy on Coronary Artery Plaque in Patients with Coronary Artery Disease: A Randomized Clinical Trial. J Am Heart Assoc. 2017; 6: e006981. 10.1161/JAHA.117.006981. https://pubmed.ncbi.nlm.nih.gov/29246960/
“High-dose eicosapentaenoic acid and docosahexaenoic acid provided additional benefit to statins in preventing progression of fibrous coronary plaque in subjects adherent to therapy with well-controlled low-density lipoprotein cholesterol levels.”
Huh JH, Jo SH. Omega-3 fatty acids and atrial fibrillation. Korean J Intern Med. 2023 May;38(3):282-289. doi: 10.3904/kjim.2022.266. Epub 2022 Dec 14. PMID: 36514212; PMCID: PMC10175873 https://pubmed.ncbi.nlm.nih.gov/36514212/
.
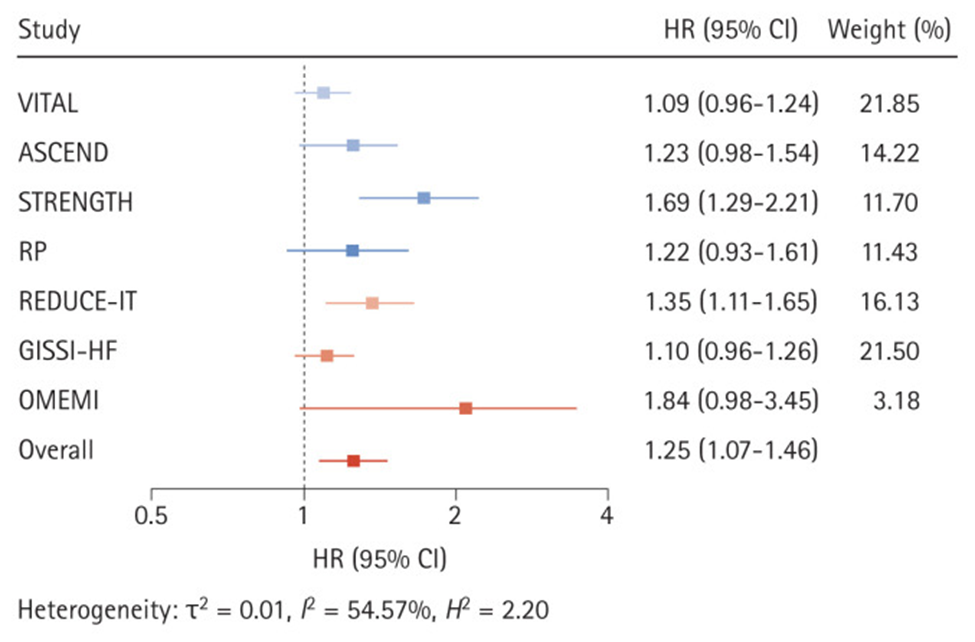
Effects of omega-3 fatty acid supplementation on the risk of atrial fibrillation. HR, hazard ratio; CI, confidence interval; VITAL, Vitamin D and Omega-3 Trial; ASCEND, A Study of Cardiovascular Events in Diabetes; STRENGTH, Statin Residual Risk with Epanova in High Cardiovascular Risk Patients with Hypertriglyceridemia; RP, Risk and Prevention Study; REDUCE-IT, Reduction of Cardiovascular Events With Icosapent Ethyl-Intervention Trial; GISSI-HF, Gruppo Italiano per lo Studio della Sopravvivenza nell’Insufficienza Cardiaca-Heart Failure; OMEMI, Omega-3 Fatty Acids in Elderly With Myocardial Infarction. Effects of omega-3 fatty acid supplementation on the risk of atrial fibrillation. HR, hazard ratio; CI, confidence interval; VITAL, Vitamin D and Omega-3 Trial; ASCEND, A Study of Cardiovascular Events in Diabetes; STRENGTH, Statin Residual Risk with Epanova in High Cardiovascular Risk Patients with Hypertriglyceridemia; RP, Risk and Prevention Study; REDUCE-IT, Reduction of Cardiovascular Events With Icosapent Ethyl-Intervention Trial; GISSI-HF, Gruppo Italiano per lo Studio della Sopravvivenza nell’Insufficienza Cardiaca-Heart Failure; OMEMI, Omega-3 Fatty Acids in Elderly With Myocardial Infarction. Effects of omega-3 fatty acid supplementation on the risk of atrial fibrillation. HR, hazard ratio; CI, confidence interval; VITAL, Vitamin D and Omega-3 Trial; ASCEND, A Study of Cardiovascular Events in Diabetes; STRENGTH, Statin Residual Risk with Epanova in High Cardiovascular Risk Patients with Hypertriglyceridemia; RP, Risk and Prevention Study; REDUCE-IT, Reduction of Cardiovascular Events With Icosapent Ethyl-Intervention Trial; GISSI-HF, Gruppo Italiano per lo Studio della Sopravvivenza nell’Insufficienza Cardiaca-Heart Failure; OMEMI, Omega-3 Fatty Acids in Elderly With Myocardial Infarction
THIS WEBSITE PROVIDES INFORMATION FOR EDUCATIONAL PURPOSES ONLY. CONSULT YOUR HEALTH CARE PROVIDER FOR MEDICAL ADVICE.
Eat clean, drink filtered water, love, laugh, exercise outdoors in a greenspace, get some morning sunlight, block the blue light before bed, engage in meaningful work, find a sense of purpose, spend time with those you love, AND sleep well tonight.
Doctor Bob