I recently gave a talk at the AHS 2022 meeting held at UCLA. You can view the video here:
The presentation covers a quick review of my presentations given last year at the PAH 2021 annual meeting (virtual) with additional information on long Covid.
Multiple nutrients acting synergistically support a balanced response to viral infections, including SARS CoV-2. Here is a picture.
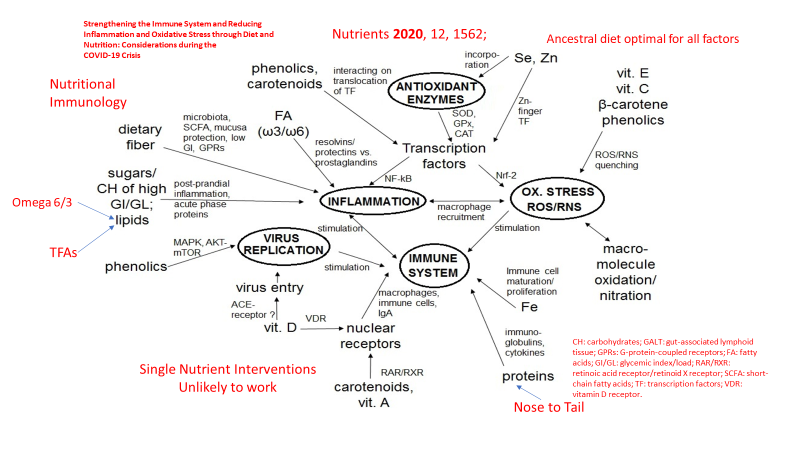
The take home message is that no single nutritional intervention is likely to have significant impact with an acute infection unless all but one nutritional component is optimal. Nevertheless, there is compelling evidence that Vitamin D deficiency is rampant in the developed world and if one nutritional intervention is likely to be of benefit, Vitamin D supplementation, particularly in high risk populations, presents the most likely candidate. As usual, preventive supplementation would be preferable to rescue high dose intervention.

In a study of frail elderly hospitalized patients, regular vitamin D supplementation was associated with decreased mortality as demonstrated here. Compared to no supplementation, regular supplementation was associated with a 93% reduction in risk of death.

A study from Spain with very high dose Vitamin D in the form of Calcifediol showed significant benefit in hospitalized patients, suggesting that Vitamin D deficiency was prevalent in that population and that such a treatment intervention should be widely considered.
Calcifediol Treatment and COVID-19-Related Outcomes
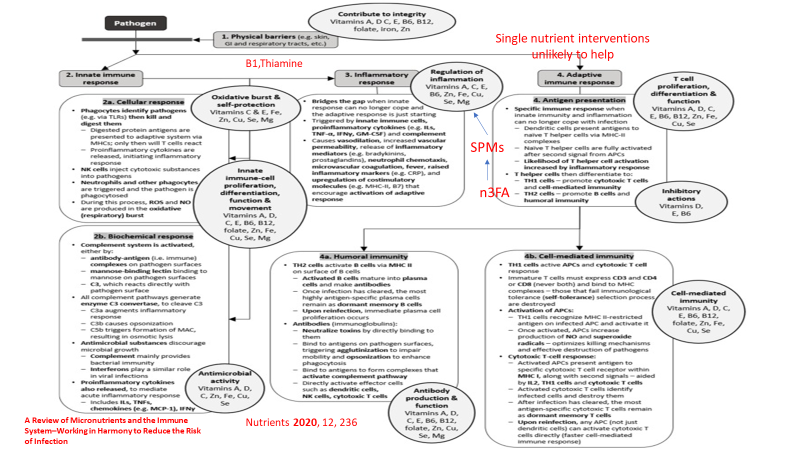
The following graphic from another nutrition review article, with red additions added by myself, demonstrates the complex interaction between nutrition and the two main components of our immune system, innate immunity (immediate response) and adaptive immunity (based on immune memory). Again red highlights added by yours truely.
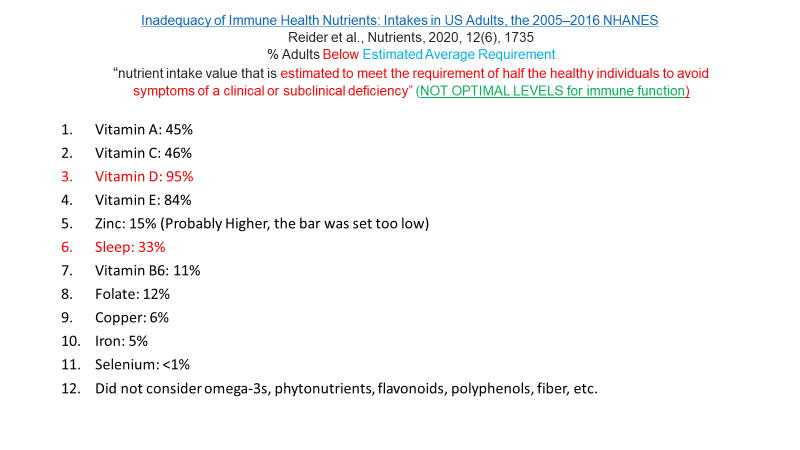
And here is a slide from my lecture with quotes from that article.

Yet most Americans are deficient in many of these essential nutrients as depicted here. The percentages represent the % of Americans that fall below the estimated amount required to prevent deficiency in HALF of adults (a very low standard).
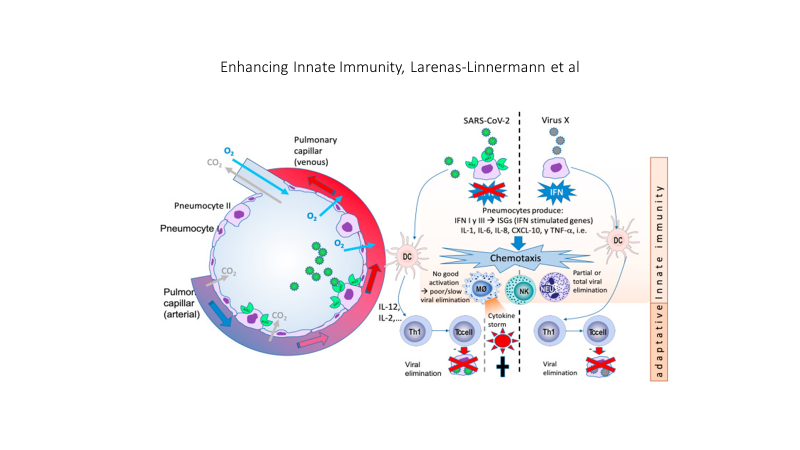
The SARS CoV2 virus interferes with a crucial component of the the initial (innate) immune response, the production of interferon 1 and the signaling of interferon one to immune cell mediators as depicted in this graphic.
Obesity, insulin and leptin resistance, also interfere with the production and signaling of interferon. The result is that people with insulin and leptin resistance (pre-diabetes, Type 2 Diabetes as well as sarcopenia) experience a double hit. First the virus itself disrupts the immune response and superimposed upon the viral effect is the effect of insulin and leptin resistance on the immune response.


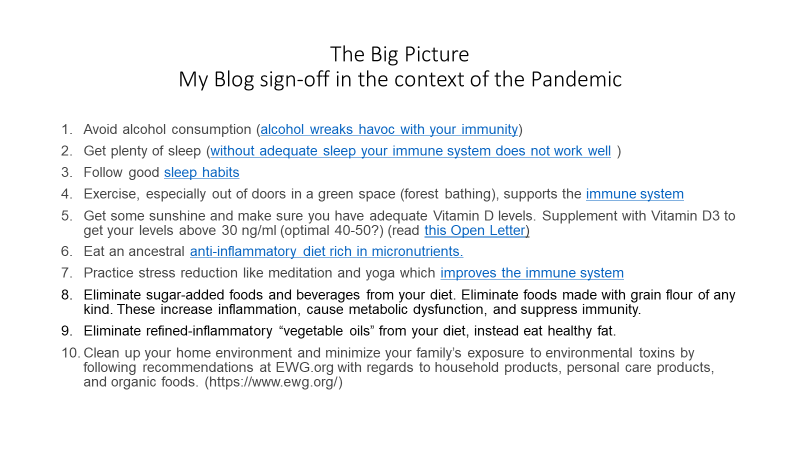
Factors that can quickly impact insulin and leptin resistance include all the components of an ancestral lifestyle depicted in my website graphic. A paleolithic or ancestral diet that eliminates sugar added foods and beverages, replacing those empty calories with nutrient dense foods, exercise, adequate restorative sleep, stress reduction, avoidance of environmental toxins, social connection. All of these affect health in general, mitigate insulin and leptin resistance, and support a balanced immune response to viral infection. The circle of health depicted below is surrounded by the many deleterious aspects of modern living. Thus, a mismatch between our evolutionary biology and present day life.

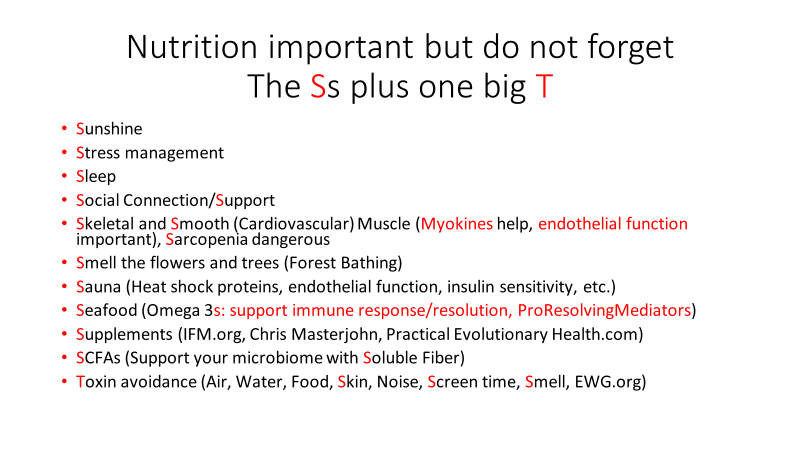
Here is a slide from my lecture that lists many lifestyle factors that can impact infection with any virus, including SARS CoV-2
My lecture also included discussion of Long COVID, theories of etiology and pathophysiology which will be discussed in my next post.
For the full lecture which is about 34 minutes long, please follow the link above.
THIS WEBSITE PROVIDES INFORMATION FOR EDUCATIONAL PURPOSES ONLY. CONSULT YOUR HEALTH CARE PROVIDER FOR MEDICAL ADVICE.
Eat clean, drink filtered water, love, laugh, exercise outdoors in a greenspace, get some morning sunlight, block the blue light before bed, engage in meaningful work, find a sense of purpose, spend time with those you love, AND sleep well tonight.
Doctor Bob
