Winter approaches with a perfect storm of 3 respiratory viruses, increased indoor activity, dry spaces, and holiday gatherings. The 3 viruses already filling many hospitals (including children’s hospitals) include RSV (Respiratory Syncytial Virus), Influenza, and SARS-CoV-2.
Respiratory viruses spread by aerosol typically enter through the nose and throat. Dry nasal and oral-pharyngeal mucosa (the lining of the nose and throat) presents an ideal incubator for respiratory viruses. With winter comes drier indoor environments created by heating systems.
Indoor conditions, particularly indoor RH (relative humidity) modulate the spread and severity of COVID-19 outbreaks.
The sweet spot was between 40% and 60% humidity to minimize spread and severity of infection.
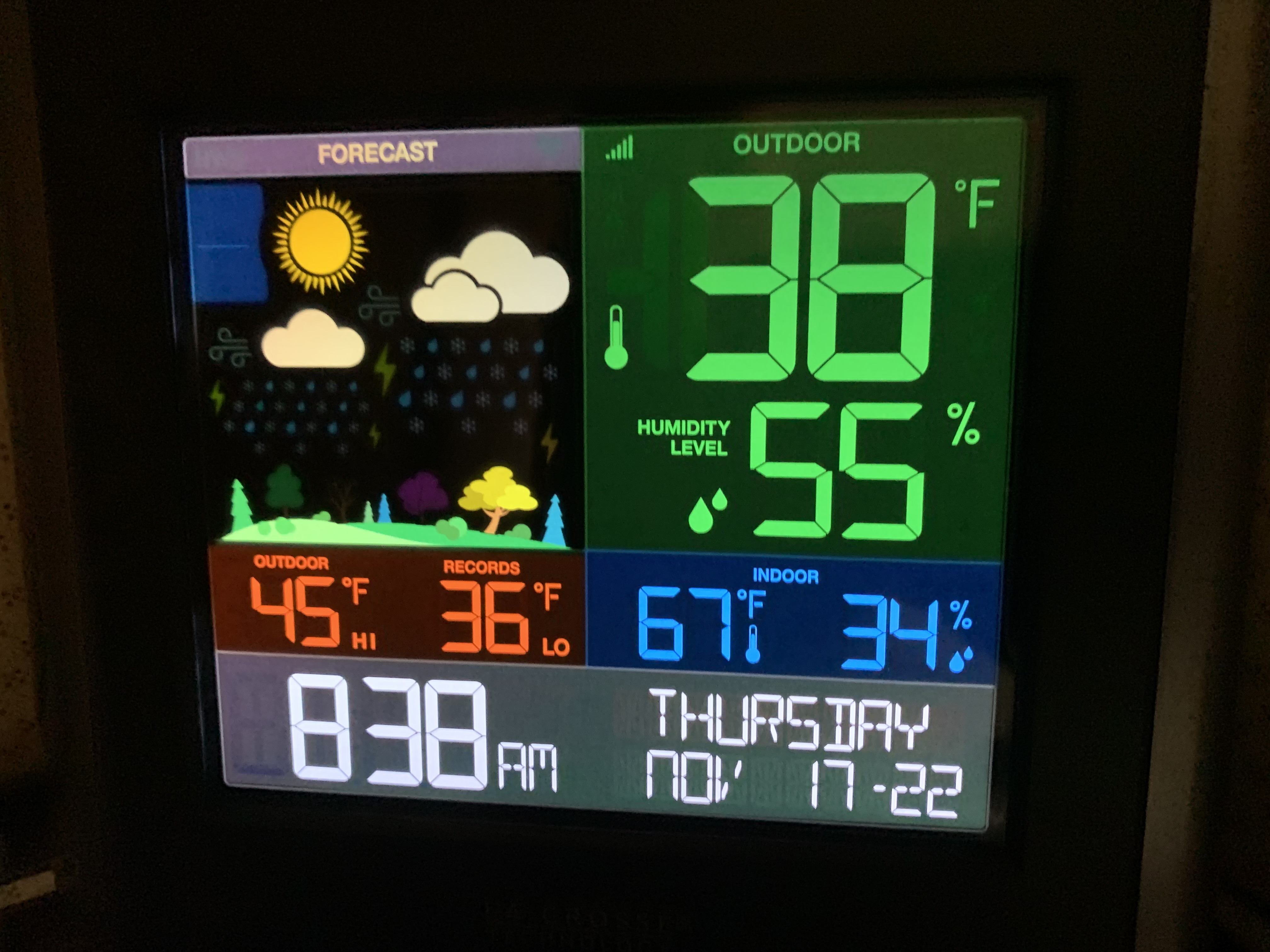
Here is a picture of the temperature and humidity monitor in my home office.
Note that while outdoor humidity is 55%, indoor humidity is only 34%, short of the “ideal” range for decreased viral transmission and severity. We have a humidifier in our bedroom where the RH is higher.
In addition to a bedroom humidifier we have several HEPA filters dispersed throughout the house. HEPA filters can decrease aerosol (viral load) by 80% or more as can the homemade Corsi-Rosenthal box. HEPA filters and the Corsi-Rosenthal Box also significantly reduce indoor air pollution, potentially protecting us from not only respiratory disease but also heart attacks, strokes, dementia and cancer.
As the winter approaches consider protecting your family and friends from RSV, Influenza, and COVID-19 by utilizing a humidifier and free standing HEPA filters. Improving indoor air quality will have many health benefits.
In the context of the COVID 19 pandemic I will close with the usual summary.
Exercise, especially out of doors in a green space, supports the immune system
Get some sunshine and make sure you have adequate Vitamin D levels. Supplement with Vitamin D3 to get your levels above 30 ng/ml, >40ng/ml arguably better.
Eliminate sugar-added foods and beverages from your diet. These increase inflammation, cause metabolic dysfunction, and suppress immunity.
Eliminate refined-inflammatory “vegetable oils” from your diet, instead eat healthy fat.
Clean up your home environment and minimize your family’s exposure to environmental toxins by following recommendations at EWG.org with regards to household products, personal care products, and organic foods. (https://www.ewg.org/)
Drink water filtered through a high quality system that eliminates most environmental toxins. (Such as a Berkey or reverse osmosis filter)
HEPA filters or the home-made version (Corsi-Rosenthal box) used in your home or workplace can reduce circulating viral load by 80%. This works for any respiratory virus transmitted by aerosol and this winter we have the triple threat of RSV, Influenza, and SARS-CoV-2. It also decreases indoor air pollution.
If you are eligible for vaccination, consider protecting yourself and your neighbor with a few jabs. Age > 50 and/or risk factors (Diabetes, pre-diabetes, insulin resistance, hypertension, obesity, heart disease, COPD, asthma, cancer treatment, immune suppression) suggests benefit from a booster. Risk for complications of boosters in adolescents, especially males, without risk factors, may equal benefit. Previous infection with Covid can be considered as protective as a booster. Discuss risk vs benefits with your doctor.
THIS WEBSITE PROVIDES INFORMATION FOR EDUCATIONAL PURPOSES ONLY. CONSULT YOUR HEALTH CARE PROVIDER FOR MEDICAL ADVICE.
Eat clean, drink filtered water, love, laugh, exercise outdoors in a greenspace, get some morning sunlight, block the blue light before bed, engage in meaningful work, find a sense of purpose, spend time with those you love, AND sleep well tonight.
This discussion was originally posted before PAXLOVID WAS AVAILABLE. The title was originally Lifestyle More Effective than Drugs.
But now we have Paxlovid. Paxlovid is very effective in reducing morbidity and mortality associated with Covid-19 infection but also appears to reduce risk of Long Covid. Standard dosing: PAXLOVID two 150-mg tablets of nirmatrelvir, one 100-mg tablet of ritonavir twice daily for 5 days.
Dose adjustments are necessary for certain medical conditions and there are many drug interactions that should be considered. But do not let that discourage you from asking your provider to prescribe this drug for an acute Covid infection. This is a truly effective drug. It decreases morbidity and mortality as well as risk for Long Covid.
The results of a randomized placebo controlled clinical trial in high risk individuals has been published in the NEJM. The study was done just when Omicron hit. The study demonstrated an 89% reduction of hospitalizations and deaths by day 28 (absolute reduction of 6.2/100) with ZERO deaths in the Paxlovid group (7 in the placebo group). Paxlovid also had LESS side effects than placebo.
Another study from Israel demonstrated equally impressive results as shown here.
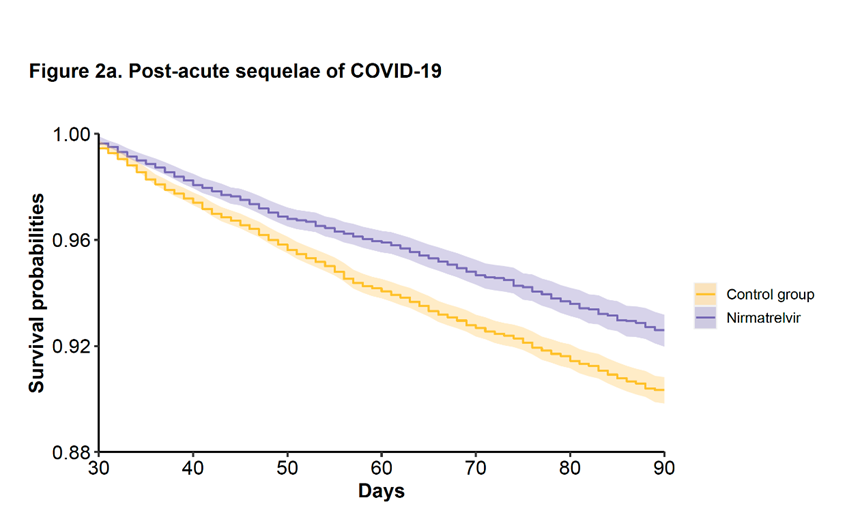
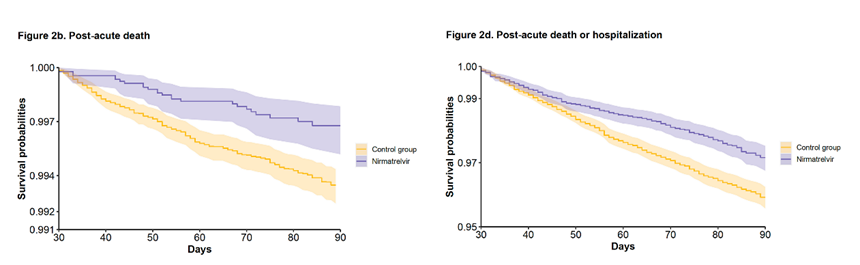
In addition, a study from the VA has looked at longer term effects (pre-print publication, still waiting for peer review.)
The study included 9000 Paxlovid patients treated within 5 days of symptom onset during the Omicron and subvariant waves and compared the treated patients with approximately 47,000 matched controls.
There was a 26% reduction in Long Covid.
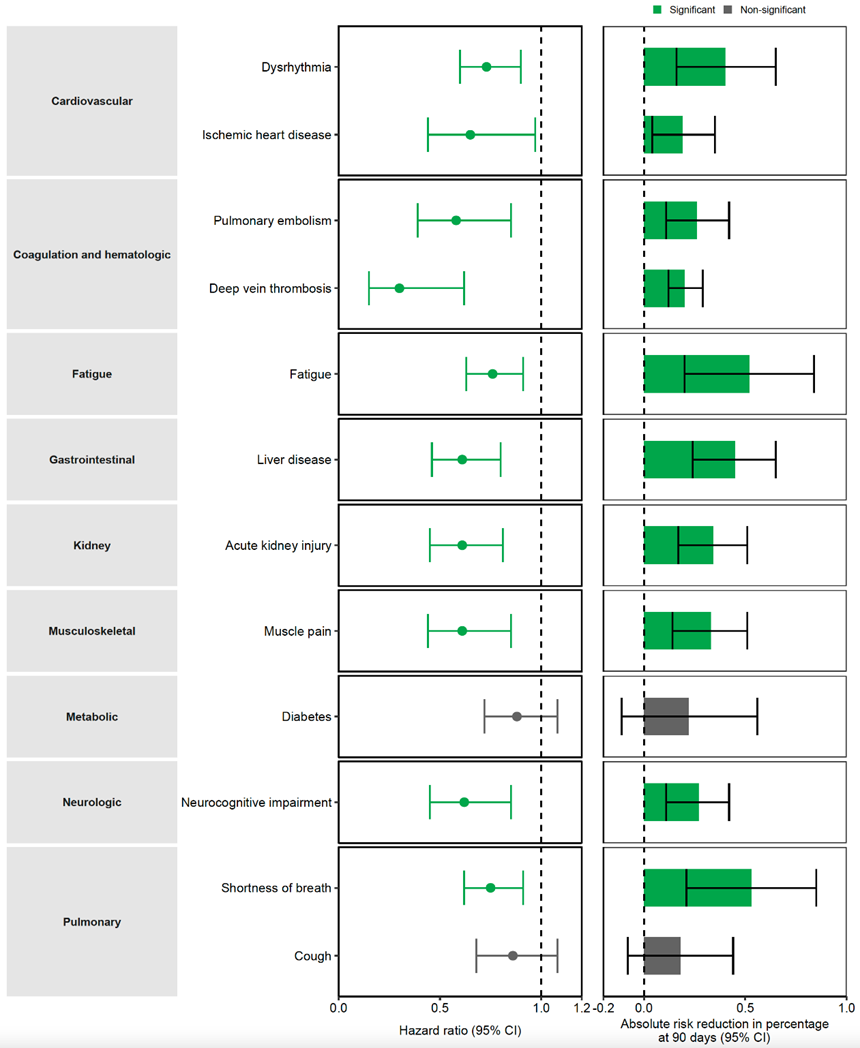
Here is a breakdown of the Long Covid Symptoms
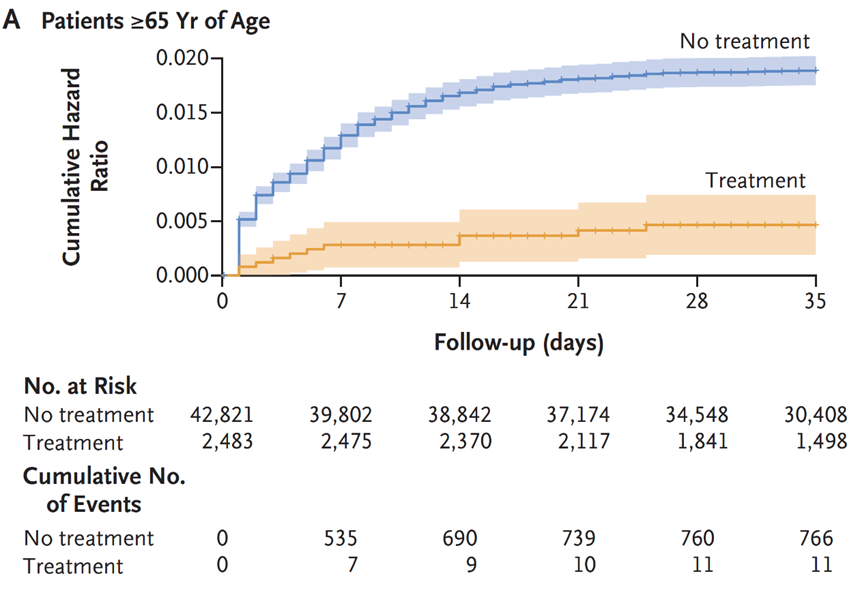
The VA study also showed a 48% reduction of death and 30% reduction in hospitalization after the acute phase (acute phase = first 30 days) as demonstrated here.
Many drug intervention trials for treating COVID-19 early in the pandemic have been disappointing. No studies have shown benefit for hydroxychloroquine, with or without azithromycin. This topic has been covered in previous posts. Remdesivir was FDA approved based upon one study that showed reduction in duration of symptoms. The mortality rate with Remdesivir, however, did not demonstrate a statistically significant difference when compared to “usual care”. https://www.niaid.nih.gov/news-events/nih-clinical-trial-shows-remdesivir-accelerates-recovery-advanced-covid-19
Another study published in Lancet failed to show any clinical benefit from Remdesivir.
“No statistically significant benefits were observed for remdesivir treatment beyond those of standard of care treatment. Our trial did not attain the predetermined sample size because the outbreak of COVID-19 was brought under control in China. Future studies of remdesivir, including earlier treatment in patients with COVID-19 and higher-dose regimens or in combination with other antivirals or SARS-CoV-2 neutralising antibodies in those with severe COVID-19 are needed to better understand its potential effectiveness.”
Likewise well designed studies of Ivermectin have shown no clinical benefit.
Monoclonal antibodies effective against early variants are no longer effective against the newer variants. So in terms of drug therapies for acute Covid infections we have Paxlovid for out patient care and dexamethasone for critically ill patients.
But we do know that certain underlying conditions such as obesity, diabetes, pre-diabetes (insulin resistance) and hypertension significantly increase risk of DEATH AND COMPLICATIONS with COVID-19. Since there are lifestyle interventions that can quickly and effectively mitigate these problems (diet, exercise, sleep, stress reduction….) now would seem like a good time to take our epidemics of obesity and diabetes in hand with aggressive lifestyle interventions to decrease the mortality rate of COVID-19 infection.
Such measures do not require expensive drugs or expensive drug trials, they simply require knowledge, guidelines and the will to implement change in our daily habits. Yet there has been little discussion about this in the media or on the part of public health officials.
Lets look at obesity in the US.
From 1999–2000 through 2017–2018, the age-adjusted prevalence of obesity increased from
30.5% to 42.4%, and the prevalence of severe obesity increased from 4.7% to 9.2%.
The most effective tool for addressing obesity and diabetes is a very low carbohydrate diet.
Effects of the Low Carbohydrate, High Fat Diet on Glycemic Control and Body Weight in Patients With Type 2 Diabetes: Experience From a Community-Based Cohort
This study was a done in a community-based program, not an academic practice setting. That is significant since it demonstrates feasibility outside of academic centers with standard community resources. The results of this study confirmed the results of many previous studies done in academic settings including better blood sugar control, reduction or elimination of diabetic medications, and significant weight loss.
“All patients following the LCHF diet who initially took insulin had either a reduction or discontinuation of this therapy by their healthcare provider when clinically indicated, compared with less than a quarter of those receiving usual care.“
In another study done in Italy, significant weight reduction (7 kg), waistline reduction (7 cm.), fat mass reduction (3.8%) and systolic blood pressure reduction (10.5 mmHg) were achieved in 3 months with a Very Low Carbohydrate diet.
Middle and Long-Term Impact of a Very Low-Carbohydrate Ketogenic Diet on Cardiometabolic Factors: A Multi-Center, Cross-Sectional, Clinical Study (https://pubmed.ncbi.nlm.nih.gov/25986079/
Nina Teicholz had an opinion piece published in the Wall Street Journal on May 30, discussing the USDA dietary guidelines that have largely ignored a massive body of evidence supporting a Very Low Carbohydrate Diet for obesity and diabetes. She cites many studies that have been ignored by the USDA dietary guidelines committee. Here is here opening statement.
“Americans with obesity, diabetes, heart disease and other diet-related diseases are about three times more likely to suffer worsened outcomes from Covid-19, including death. Had we flattened the still-rising curves of these conditions, it’s quite possible that our fight against the virus would today look very different.”
But think about that simple statement, THREE TIMES MORE LIKELY TO SUFFER WORSENED OUTCOMES FROM COVID-19. Yet these conditions are highly responsive to lifestyle interventions that not only mitigate obesity, insulin resistance and high blood pressure, but also enhance immune function.
More from Teicholz’s opinion piece:
“Other studies have found that dietary changes can rapidly and substantially improve cardiovascular risk factors, including conditions like hypertension that are major risk factors for worsened Covid-19 outcomes. A 2011 study in the journal Obesity on 300 clinic patients eating a very low-carbohydrate diet saw blood pressure quickly drop and remain low for years. And a 2014 trial on 148 subjects, funded by the National Institutes of Health, found a low-carb diet to be “more effective for weight loss and cardiovascular risk factor reduction” than a low-fat control diet at the end of the 1-year experiment.“
In a recent letter to the editor published in the journal METABOLISM, Dr. Casey Means points out:
A diagnosis of diabetes has been a key indicator of the severity of COVID-19, and in this regard, the virus has relentlessly highlighted our global Achilles heel of metabolic dysfunction, and points to a prime opportunity to fight back. That fight, however, is not going to be won with Clorox, Purell, masks, or anti-IL-6 drugs. The fight will only be won through a serious commitment to improving everyone’s foundational metabolic health, starting with the lowest hanging evidence-based fruit: dietary and lifestyle interventions.
In 2 pages the letter describes multiple benefits of better glucose control relative to COVID -19 infection and the immune system as well as reduction of factors that lead to cytokine storm (terminal event for many COVID-19 patients). The letter also discusses the benefit of reducing environmental toxins (discussed in previous posts about COVID-19 and other health problems) that would likely benefit COVID-19 patients.
Research published April 18th, 2020 found that patients exposed to highest amount of environmental nitrogen dioxide (NO2) had increased risk of death fromCOVID-19, and that long-term exposure to this pollutant may be one of the most important contributors to fatality by compounding lung inflammation [20].
Minimizing exposure to environmental pollutants may serve a role in quelling the underlying pro-inflammatory state that characterizes metabolic disease and COVID-19 associated cytokine storms.
Other environmental toxins, including persistent organic pollutants (POPs) found in air, water, and food generated from pesticides and industrial chemicals, are also strongly implicated in the pathogenesis of metabolic syndrome; promoting “clean living,” toxin-avoidant strategies for patients as simple as emphasizing organic foods, home air purification, and non-toxic home supplies could be considered, although the clinical utility of these measures in the acute setting is unknown [21].
In discussing the white elephant in the room he states:
What is starkly missing is the clear, simple, and strong recommendation for no added sugar or ultra-refined carbohydrates, both of which are known drivers of postprandial hyperglycemia and inflammation. As a medical community, we must not miss the opportunity to serve patients with straightforward, evidence-based nutritional and lifestyle strategies to assist in glycemic control.
I would encourage you to follow the link and read the 2 pages supported by multiple peer-reviewed references.
An ancestral (paleo) diet is also very effective for addressing insulin resistance, diabetes type 2 and obesity. Multiple studies have demonstrated this. Although an ancestral approach is typically low carb it is not typically ketogenic, but a ketogenic ancestral diet (high in non starchy vegetables to support the gut microbiome) can be implemented by restricting fruits to one serving of berries per day and limiting starchy vegetables.
Even without severe carbohydrate restriction, an ancestral anti-inflammatory diet will quickly address insulin resistance, type 2 diabetes, and obesity. In this study, insulin resistance was reversed in 10 days.
And another study compared an Ancestral (Paleo) diet to the Mediterranean diet in patients with ischemic heart disease AND insulin resistance (glucose intolerance or type 2 diabetes). Ancestral diet was superior to the Mediterranean diet in improving insulin sensitivity, blood sugar control and greater fat loss. Fasting blood sugars normalized in all patients on the Ancestral diet who had previously had abnormal blood sugars.
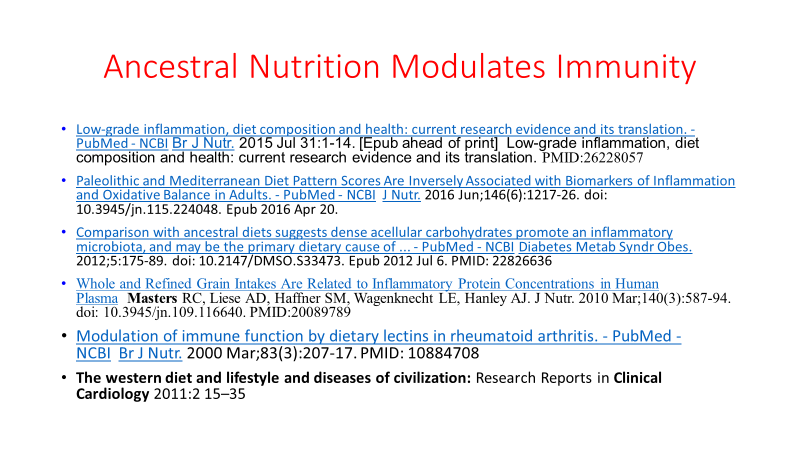
And here is a slide from one of my lectures with references on how an ancestral diet modulates immunity.
Leptin resistance, insulin resistance and obesity travel together. Here is yet another study demonstrating the effectiveness of an ancestral diet.
If you have obesity, diabetes or pre-diabetes the Very Low Carbohydrate version of the anti-inflammatory diet linked above would be the fastest and most effective intervention you can immediately employ to reduce your risk of succumbing to COVID-19. (Of course wear an N-95, follow good hygiene with hand-washing frequently, and use a HEPA filter or Corsi-Rosenthal box in your home, office, and enclosed work spaces)
In the context of the COVID 19 pandemic I will close with the usual summary.
Exercise, especially out of doors in a green space, supports the immune system
Get some sunshine and make sure you have adequate Vitamin D levels. Supplement with Vitamin D3 to get your levels above 30 ng/ml, >40ng/ml arguably better.
Eliminate sugar-added foods and beverages from your diet. These increase inflammation, cause metabolic dysfunction, and suppress immunity.
Eliminate refined-inflammatory “vegetable oils” from your diet, instead eat healthy fat.
Clean up your home environment and minimize your family’s exposure to environmental toxins by following recommendations at EWG.org with regards to household products, personal care products, and organic foods. (https://www.ewg.org/)
Drink water filtered through a high quality system that eliminates most environmental toxins.
If you are eligible for vaccination, consider protecting yourself and your neighbor with a few jabs. Age > 50 and/or risk factors (Diabetes, pre-diabetes, insulin resistance, hypertension, obesity, heart disease, COPD, asthma, cancer treatment, immune suppression) suggests benefit from a booster. Risk for complications of boosters in adolescents, especially males, without risk factors, may equal benefit. Previous infection with Covid can be considered as protective as a booster. Discuss risk vs benefits with your doctor.
THIS WEBSITE PROVIDES INFORMATION FOR EDUCATIONAL PURPOSES ONLY. CONSULT YOUR HEALTH CARE PROVIDER FOR MEDICAL ADVICE.
Eat clean, drink filtered water, love, laugh, exercise outdoors in a greenspace, get some morning sunlight, block the blue light before bed, engage in meaningful work, find a sense of purpose, spend time with those you love, AND sleep well tonight.
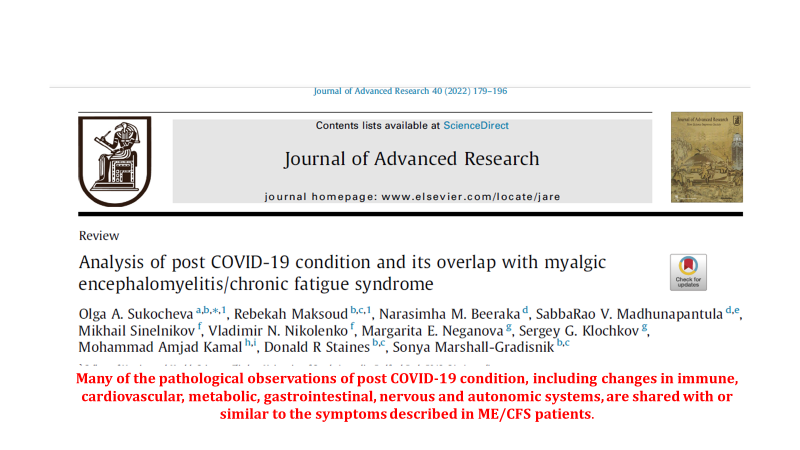
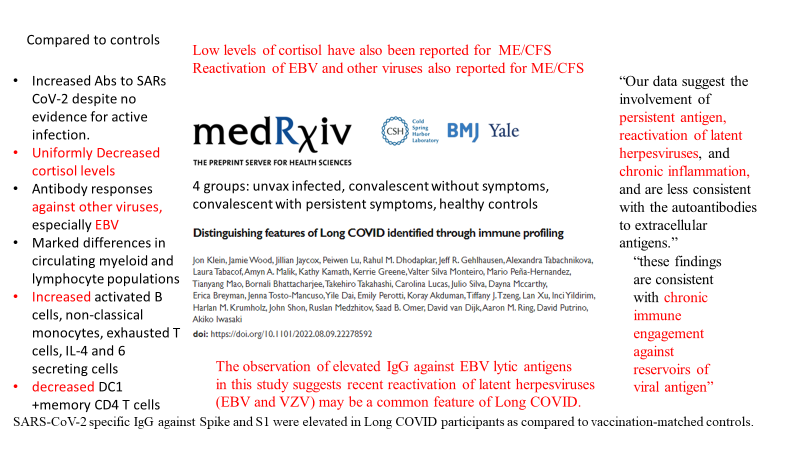
There is great overlap in symptoms and physiology of Long Covid and ME/CFS (Myalgic Encephalitis/Chronic Fatigue Syndrome.
Both are marked by Brain Fog, Cognitive Impairment, Post Exertional Malaise, with similar findings on studies of the immune system and the neuro-endocrine system in these conditions.
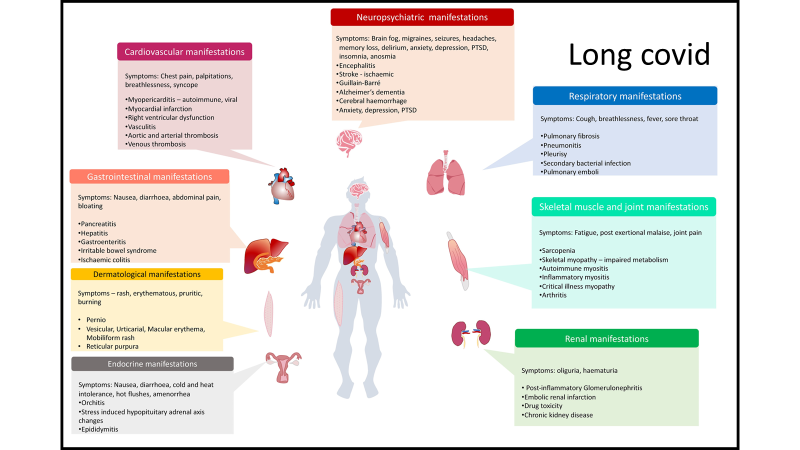
Here is a picture of organ involvement with CFS:
And here is a picture of Long Covid.
Do you notice the similarities and overlap?
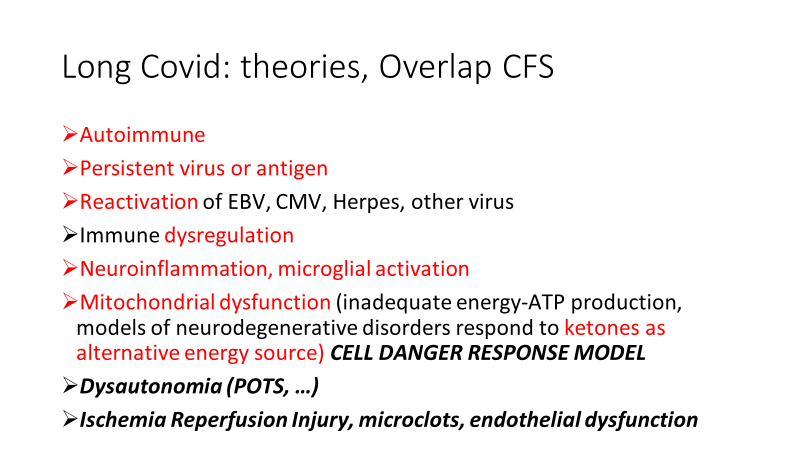
The theories/clinical findings of studies regarding both have overlap:
Low Dose Naltrexone has been studied for many chronic ailments in small studies. Since this is available in generic form there are no big profits to be made by the pharmaceutical industry so do not expect large studies with this medication. (I wish NIH would get on the ball and fund studies of this and other interventions utilizing nutraceuticals such as Rhodiola).
Here is a very hopeful study with regards to Long Covid and Low Dose Naltrexone.
Recovery from symptoms, activities of daily living, energy level, pain, concentration, sleep quality and mood ALL IMPROVED!
If this were a patented drug it would be a BLOCKBUSTER for a pharmaceutical company.
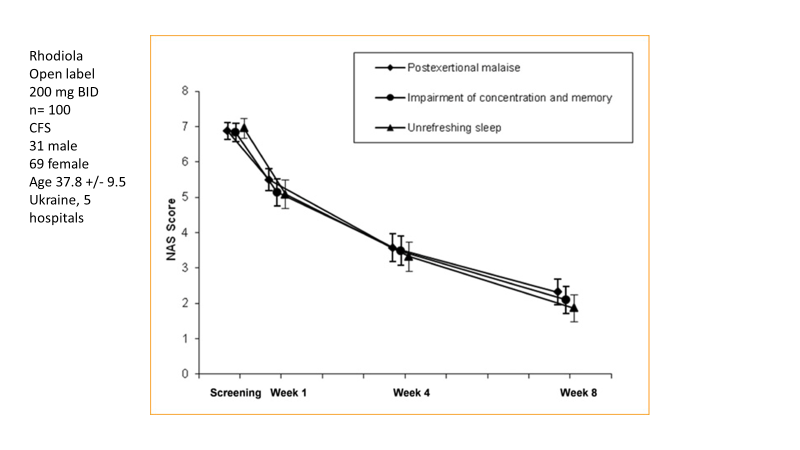
And since Chronic Fatigue Syndrome represents a major portion of Long Covid patients, pathophysiology AND symptoms, here is a study of an adaptogen called Rhodiola (a plant nutraceutical in the category of ADAPTOGEN).
Look at the amazing improvement in major components of CFS/ME which represent the major complaints of many patients with Long Covid.
Post Exertional Malaise, Concentration, Memory and Sleep ALL IMPROVED by more than 50% within eight weeks.
But this is an over the counter supplement, so again, no big profits for big pharma.
You will note the diversity of clinical applications for Low Dose Naltrexone including autoimmune disease (one possible mechanism of long Covid), neuro-inflammation (another probable mechanism of Long Covid and ME-CFS).
In the context of the COVID 19 pandemic I will close with the usual summary.
Exercise, especially out of doors in a green space, supports the immune system
Get some sunshine and make sure you have adequate Vitamin D levels. Supplement with Vitamin D3 to get your levels above 30 ng/ml, >40ng/ml arguably better.
Eliminate sugar-added foods and beverages from your diet. These increase inflammation, cause metabolic dysfunction, and suppress immunity.
Eliminate refined-inflammatory “vegetable oils” from your diet, instead eat healthy fat.
Clean up your home environment and minimize your family’s exposure to environmental toxins by following recommendations at EWG.org with regards to household products, personal care products, and organic foods. (https://www.ewg.org/)
Drink water filtered through a high quality system that eliminates most environmental toxins.
If you are eligible for vaccination, consider protecting yourself and your neighbor with a few jabs. Age > 50 and/or risk factors (Diabetes, pre-diabetes, insulin resistance, hypertension, obesity, heart disease, COPD, asthma, cancer treatment, immune suppression) suggests benefit from a booster. Risk for complications of boosters in adolescents, especially males, without risk factors, may equal benefit. Previous infection with Covid can be considered as protective as a booster. Discuss risk vs benefits with your doctor.
THIS WEBSITE PROVIDES INFORMATION FOR EDUCATIONAL PURPOSES ONLY. CONSULT YOUR HEALTH CARE PROVIDER FOR MEDICAL ADVICE.
Eat clean, drink filtered water, love, laugh, exercise outdoors in a greenspace, get some morning sunlight, block the blue light before bed, engage in meaningful work, find a sense of purpose, spend time with those you love, AND sleep well tonight.
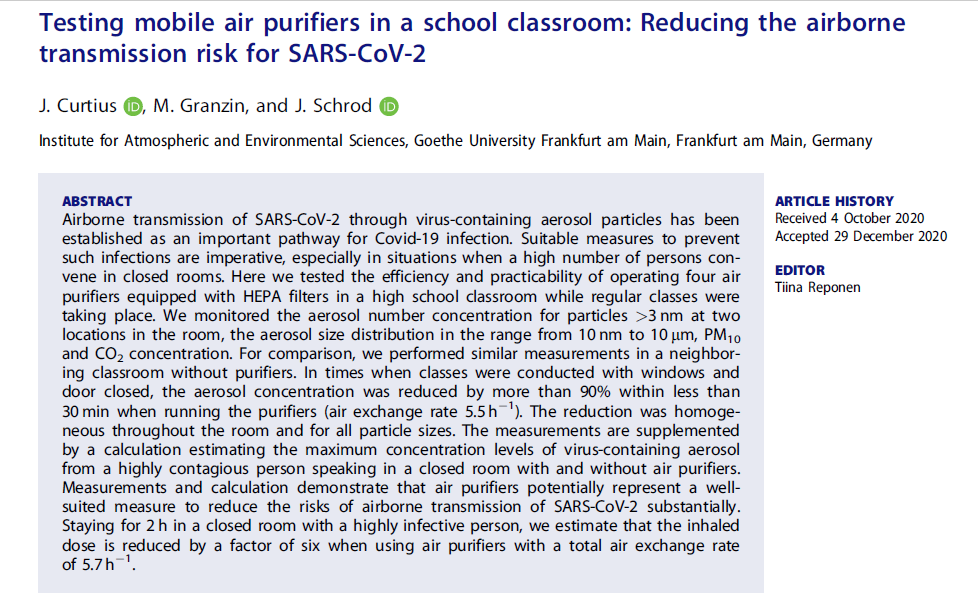
SARS CoV-2 virus is spread by aerosols. These aerosols contain many viruses carried in a tiny amount of liquid from a person’s mouth and nose as they breath, talk, sing, or yell. Yelling, singing, coughing, sneezing produce more aerosol than breathing. Risk of transmission in a room depends on duration of exposure (time in the room), amount of ventilation, # of individuals carrying the virus present and their activity . A 5 micron aerosol can stay suspended in air for 30 minutes indoors.
HEPA filters (High Efficiency Powered Air-filters) can dramatically reduce the number of aerosols in a room. This includes not only virus carrying aerosols but also small particulate pollutants, both of which impact the health and safety of children and adults in classrooms, meeting rooms and businesses.
HEPA filters range in price from $150 to $800 or more depending on quality, efficiency and how quiet they run. They have been tested in classrooms and hospitals.
In the hospital setting they have dramatically decreased COVID Virus.
To determine how the filters stand up to real-world conditions, Navapurkar and his co-authors installed them in two fully occupied COVID-19 wards — a general ward and an ICU. The team chose high-efficiency particulate air (HEPA) filters, which blow air through a fine mesh that catches extremely small particles. The researchers collected air samples from the wards during a week when the air filters were switched on and two weeks when they were turned off.
In the general ward, the team found SARS-CoV-2 particles in the air when the filter was off but not when it was on. Surprisingly, the team didn’t find many viral particles in the air of the ICU ward, even when the filter there was off. The authors suggest several possible reasons for this, including slower viral replication at later stages of the disease3. As a result, the team says that measures to remove the virus from the air might be more important in general wards than in ICUs.
An Engineering professor and Dean at UC Davis, Richard Corsi, tweeted the design of an inexpensive homemade air filter providing the equivalent aerosol clearing capacity as an expensive manufactured HEPA filter. A colleague in Texas built one with simple components from a hardware store. The result was called the Corsi-Rosenthal box.
Made with four MERV 13 Airfilters, a box fan , duct tape and cardboard.
Dr. Corsi is an expert in the engineering of HVAC systems. He has researched methods to improve indoor air quality and published many scientific studies involving the interaction between pollutants and indoor materials. He estimates that the cost of a home-made Corsi-Rosenthal box is $4.50 per year per student to build and run based on average class size in the US. These are easily made with simple components and instructions available on-line. In fact if you search YouTube you will find many short videos on how to build these in 20 minutes. Their construction and use could easily be a classroom activity.
Here is a picture of the Corsi-Rosenthal box from Wikipedia:
One box can help to improve the air quality in an average size classroom, offering the equivalent of 7 to 8 air changes an hour.
These boxes would not only benefit health by decreasing circulating virus containing aerosols but also filtering out indoor pollutants that come from latex paint, carpet fibers, cleaning chemicals, air fresheners, fire retardants on furniture and clothing, which all release volatile organic compounds (VOCs) that cause lung damage, increase risk of asthma and autoimmune disease. So why have these not been widely used in our schools, homes, and businesses?
Why has the CDC not recommended this simple and inexpensive highly effective risk reduction approach? If widely implemented soon after Drs. Corsi and Rosenthal invented and advocated it’s use, it would have prevented many infections and allayed some of the fear and anxiety of teachers, students and parents. As the flu season approaches, and with the added risk of a triple threat presented by RSV, Influenza, and Covid, all transmitted by aerosol, now would be a great time to build some for your home, business, office or your chidren’s school classrooms.
In the context of the COVID 19 pandemic I will close with the usual summary.
Exercise, especially out of doors in a green space, supports the immune system
Get some sunshine and make sure you have adequate Vitamin D levels. Supplement with Vitamin D3 to get your levels above 30 ng/ml, >40ng/ml arguably better.
Eliminate sugar-added foods and beverages from your diet. These increase inflammation, cause metabolic dysfunction, and suppress immunity.
Eliminate refined-inflammatory “vegetable oils” from your diet, instead eat healthy fat.
Clean up your home environment and minimize your family’s exposure to environmental toxins by following recommendations at EWG.org with regards to household products, personal care products, and organic foods. (https://www.ewg.org/)
Drink water filtered through a high quality system that eliminates most environmental toxins.
If you are eligible for vaccination, consider protecting yourself and your neighbor with a few jabs. Age > 50 and/or risk factors (Diabetes, pre-diabetes, insulin resistance, hypertension, obesity, heart disease, COPD, asthma, cancer treatment, immune suppression) suggests benefit from a booster. Risk for complications of boosters in adolescents, especially males, without risk factors, may equal benefit. Previous infection with Covid can be considered as protective as a booster. Discuss risk vs benefits with your doctor.
THIS WEBSITE PROVIDES INFORMATION FOR EDUCATIONAL PURPOSES ONLY. CONSULT YOUR HEALTH CARE PROVIDER FOR MEDICAL ADVICE.
Eat clean, drink filtered water, love, laugh, exercise outdoors in a greenspace, get some morning sunlight, block the blue light before bed, engage in meaningful work, find a sense of purpose, spend time with those you love, AND sleep well tonight.
An excellent article recently published in the Atlantic was so well written that I have cut and pasted important snippets to help create this post. The review confirms many findings uncovered in my reading of several scientific publications.
20 to 30 percent of patients report brain fog three months after their initial infection, as do 65to85 percent of the long-haulers who stay sick for much longer.
Of long COVID’s many possible symptoms, brain fog “is by far one of the most disabling and destructive,”
It is more profound than the clouded thinking that accompanies hangovers, stress, or fatigue.
It is almost always a disorder of “executive function”—the set of mental abilities that includes:
focusing attention,
holding information in mind, and
blocking out distractions.
Patients state they often lose focus mid-sentence.
Difficulty with simple tasks impairs activities of daily living.
“I couldn’t unload a dishwasher, because identifying an object, remembering where it should go, and putting it there was too complicated.”
The memories are there, but with impaired executive function, the brain neither chooses the important things to store nor retrieves that information efficiently.
Most people with brain fog are not so severely affected, and gradually improve with time. But even when people recover enough to work, they can struggle with minds that are less nimble than before.
“I’ve had surgeons who can’t go back to surgery, because they need their executive function,” Monica Verduzco-Gutierrez, a rehabilitation specialist at UT Health San Antonio.
That specific constellation of problems also befalls many people living with HIV, epileptics after seizures, cancer patients experiencing so-called chemo brain, and people with several complex chronic illnesses such as fibromyalgia.
People with brain fog also excel at hiding it: to protect their jobs when still able to work, or to protect their reputation, or out of embarrassment.
“I know my value in many people’s eyes will be diminished by knowing that I have these cognitive challenges.”
Individuals with previously above average cognitive ability often test “normal” but suffer significant loss compared to their prior ability.
A team of British researchers analyzed data from the UK Biobank study. The findings revealed structural changes in the brain with loss of tissue on MRI scans that correlates with symptoms.
They found that even mild infections can slightly shrink the brain and reduce the thickness of its neuron-rich gray matter. At their worst, these changes were comparable to a decade of aging.
They were especially pronounced in areas such as the parahippocampal gyrus, which is important for encoding and retrieving memories, and the orbitofrontal cortex, which is important for executive function.
In most cases the virus probably harms the brain without directly infecting it.
Inflammatory chemicals can travel from the lungs to the brain, where they disrupt cells called microglia (immune cells in the brain).
In their presence, the hippocampus—a region crucial for memory—produces fewer fresh neurons, while many existing neurons lose their insulating coats (demyelination), so electric signals now course along these cells more slowly.
These are the same changes seen in cancer patients with “chemo fog”.
Neuro-inflammation is “probably the most common way” that COVID results in brain fog, but that there are likely many such routes, such as reactivation of dormant viruses such as Epstein-Barr virus, which has been linked to conditions including ME/CFS and multiple sclerosis.
These problems can be exacerbated or mitigated by factors such as sleep and rest, which explains why many people with brain fog have good days and bad days.
Although other respiratory viruses can wreak inflammatory havoc on the brain, SARS-CoV-2 does so more potentlythan influenza.
For adults following SARS CoV-2 infection:
risks of cognitive deficit (known as brain fog), dementia, psychotic disorders, and epilepsy or seizures were still increased at the end of the 2-year follow-up period.
For children following SARS CoV-2 infection:
in the 6 months after SARS-CoV-2 infection, children were not at an increased risk of mood (HR 1·02 [95% CI 0·94–1·10) or anxiety (1·00 [0·94–1·06]) disorders, but did have an increased risk of cognitive deficit, insomnia, intracranial haemorrhage, ischaemic stroke, nerve, nerve root, and plexus disorders, psychotic disorders, and epilepsy or seizures (HRs ranging from 1·20 [1·09–1·33] to 2·16 [1·46–3·19])…. Unlike adults, cognitive deficit in children had a finite risk horizon (75 days) and a finite time to equal incidence (491 days).
The fact that neurological and psychiatric outcomes were similar during the delta and omicron waves indicates that the burden on the health-care system might continue even with variants that are less severe in other respects.
There are no proven drug treatments for long-haulers.
But there is hope.
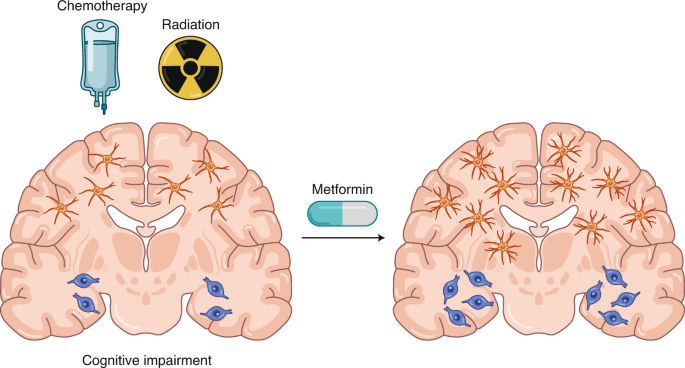
Cancer researchers have developed drugs that can calm inflamed microglia in mice and restore their cognitive abilities;
“Metformin can promote the regeneration of neural precursor cell populations and improve cognitive function in a preclinical model of cranial radiation and a pilot clinical study of children after cranial radiation and chemotherapy.”
With regard to long-haulers, better sleep, healthy eating, and other generic lifestyle changes can make the condition more tolerable. Breathing and relaxation techniques can help people through bad flare-ups; speech therapy can help those with problems finding words.
“Some people spontaneously recover back to baseline,”
The largest group of long-haulers—those whose brain fog has improved but not vanished, can “maintain a relatively normal life, but only after making serious accommodations,”
Patients struggle to make peace with how much they’ve changed and the stigma associated with it, regardless of where they end up.
People with ME/CFS learned this lesson the hard way, and fought hard to get exercise therapy, once commonly prescribed for the condition, to be removed from official guidance in the U.S. and U.K.
In summary:
Brain fog can occur even after mild or asymptomatic Covid-19.
Although many patients improve over time, many are left with disability that can range from mild to incapacitating.
Although these symptoms can occur following any viral infection, SARS CoV-2 seems to produce this with greater frequency compared to other viruses.
Chronic brain inflammation is the likely cause in many individuals.
Reactivation of Epstein Barr and/or other dormant viruses is suggested by various immune markers.
The immune signature also suggests an immune response that mimics persistent infection in the absence of live SARS CoV-2 virus.
Post exertional malaise following physical or mental exercise is a common and debilitating symptom without proven treatments. However there are guidelines that may help mitigate this devastating condition.
Exercise, especially out of doors in a green space, supports the immune system
Get some sunshine and make sure you have adequate Vitamin D levels. Supplement with Vitamin D3 to get your levels above 30 ng/ml, >40ng/ml arguably better.
Eliminate sugar-added foods and beverages from your diet. These increase inflammation, cause metabolic dysfunction, and suppress immunity.
Eliminate refined-inflammatory “vegetable oils” from your diet, instead eat healthy fat.
Clean up your home environment and minimize your family’s exposure to environmental toxins by following recommendations at EWG.org with regards to household products, personal care products, and organic foods. (https://www.ewg.org/)
Drink water filtered through a high quality system that eliminates most environmental toxins.
If you are eligible for vaccination, consider protecting yourself and your neighbor with a few jabs. Age > 50 and/or risk factors means clear benefit from a booster.
THIS WEBSITE PROVIDES INFORMATION FOR EDUCATIONAL PURPOSES ONLY. CONSULT YOUR HEALTH CARE PROVIDER FOR MEDICAL ADVICE.
Eat clean, drink filtered water, love, laugh, exercise outdoors in a greenspace, get some morning sunlight, block the blue light before bed, engage in meaningful work, find a sense of purpose, spend time with those you love, AND sleep well tonight.
I recently gave a talk at the AHS 2022 meeting held at UCLA. You can view the video here:
This first slide gives a good overview.
The presentation covers a quick review of my presentations given last year at the PAH 2021 annual meeting (virtual) with additional information on long Covid.
Multiple nutrients acting synergistically support a balanced response to viral infections, including SARS CoV-2. Here is a picture.
The take home message is that no single nutritional intervention is likely to have significant impact with an acute infection unless all but one nutritional component is optimal. Nevertheless, there is compelling evidence that Vitamin D deficiency is rampant in the developed world and if one nutritional intervention is likely to be of benefit, Vitamin D supplementation, particularly in high risk populations, presents the most likely candidate. As usual, preventive supplementation would be preferable to rescue high dose intervention.
In a study of frail elderly hospitalized patients, regular vitamin D supplementation was associated with decreased mortality as demonstrated here. Compared to no supplementation, regular supplementation was associated with a 93% reduction in risk of death.
A study from Spain with very high dose Vitamin D in the form of Calcifediol showed significant benefit in hospitalized patients, suggesting that Vitamin D deficiency was prevalent in that population and that such a treatment intervention should be widely considered.
Calcifediol Treatment and COVID-19-Related Outcomes
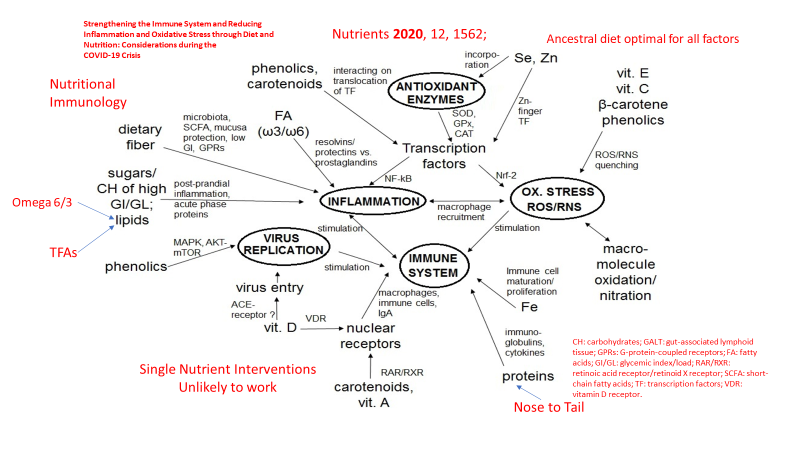
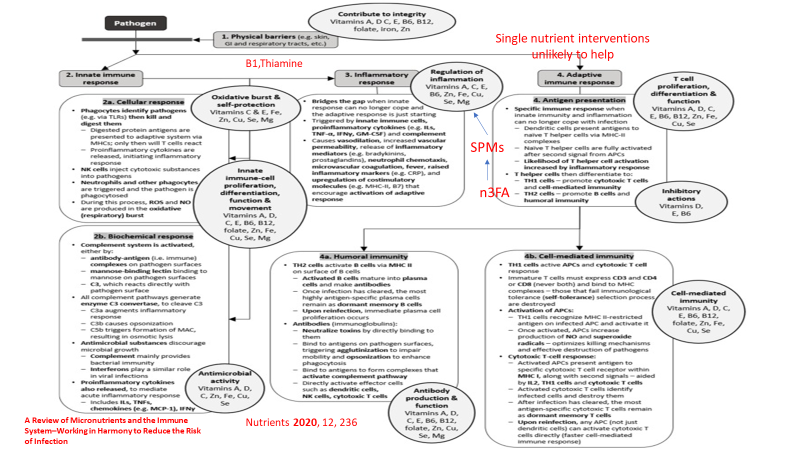
The following graphic from another nutrition review article, with red additions added by myself, demonstrates the complex interaction between nutrition and the two main components of our immune system, innate immunity (immediate response) and adaptive immunity (based on immune memory). Again red highlights added by yours truely.
And here is a slide from my lecture with quotes from that article.
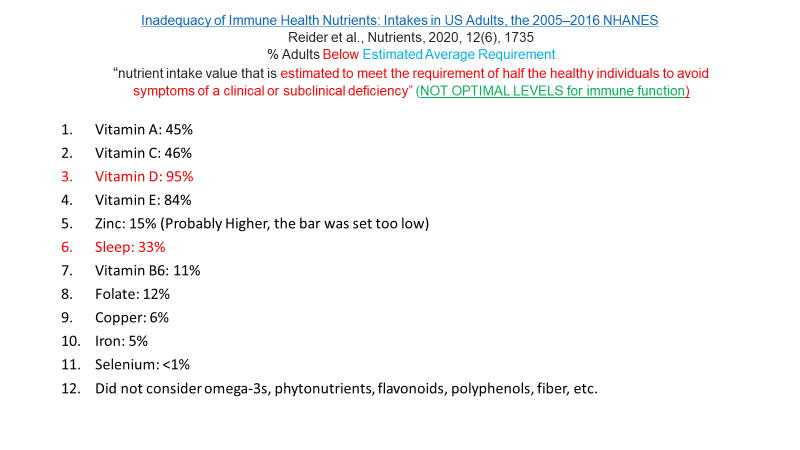
Yet most Americans are deficient in many of these essential nutrients as depicted here. The percentages represent the % of Americans that fall below the estimated amount required to prevent deficiency in HALF of adults (a very low standard).
The EAR is a very low bar to meet, yet many Americans fall below even that low standard.
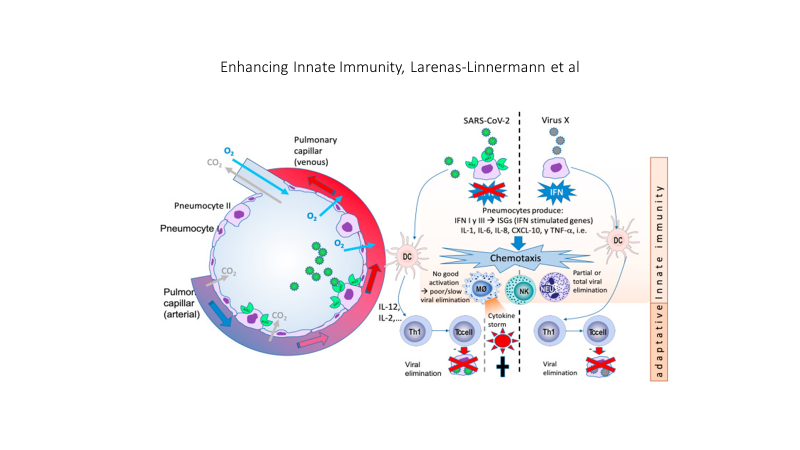
The SARS CoV2 virus interferes with a crucial component of the the initial (innate) immune response, the production of interferon 1 and the signaling of interferon one to immune cell mediators as depicted in this graphic.
SARS CoV2 on the left is compared to Virus X on the right. On the left interferon 1 (IFN) production and signaling is blocked by the virus, interfering with an effective and controlled immune response, on the right IFN is not blocked. A cascade of events results in TOO LITTLE, TOO LATE, AND THEN TOO MUCH of an immune response, producing a cytokine storm.
Obesity, insulin and leptin resistance, also interfere with the production and signaling of interferon. The result is that people with insulin and leptin resistance (pre-diabetes, Type 2 Diabetes as well as sarcopenia) experience a double hit. First the virus itself disrupts the immune response and superimposed upon the viral effect is the effect of insulin and leptin resistance on the immune response.
SOCS: suppressor of cytokine signaling. Several recent viral studies have shown that viral genes can hijack SOCS1 to inhibit host antiviral pathways, as a strategy to evade host immunityOn the left Interferon production and signaling are normal and a successful immune response is mounted. On the right the presence of insulin and leptin resistance, associated with obesity results in an initial inadequate response and a late excessive response. TOO LITTLE, TOO LATE, THEN TOO MUCH.
Factors that can quickly impact insulin and leptin resistance include all the components of an ancestral lifestyle depicted in my website graphic. A paleolithic or ancestral diet that eliminates sugar added foods and beverages, replacing those empty calories with nutrient dense foods, exercise, adequate restorative sleep, stress reduction, avoidance of environmental toxins, social connection. All of these affect health in general, mitigate insulin and leptin resistance, and support a balanced immune response to viral infection. The circle of health depicted below is surrounded by the many deleterious aspects of modern living. Thus, a mismatch between our evolutionary biology and present day life.
Here is a slide from my lecture that lists many lifestyle factors that can impact infection with any virus, including SARS CoV-2
My lecture also included discussion of Long COVID, theories of etiology and pathophysiology which will be discussed in my next post.
For the full lecture which is about 34 minutes long, please follow the link above.
THIS WEBSITE PROVIDES INFORMATION FOR EDUCATIONAL PURPOSES ONLY. CONSULT YOUR HEALTH CARE PROVIDER FOR MEDICAL ADVICE.
Eat clean, drink filtered water, love, laugh, exercise outdoors in a greenspace, get some morning sunlight, block the blue light before bed, engage in meaningful work, find a sense of purpose, spend time with those you love, AND sleep well tonight.
I will be presenting at the next Ancestral Health Symposium, at UCLA, on August 18. The title of my talk will be:
Nutritional and Lifestyle Immunology related to Acute and Long Covid.
AHS includes talks, posters, movement sessions, workshops, and a welcome dinner.
It is a scientific conference but is generally lay-accessible.
AHS covers a wide range of topics, from diet to sleep, breathing, movement, and more — all examined through the lens of evolutionary mismatch
AHS examines various ways modern human life has diverged from how we evolved successfully for millennia and how those differences are affecting us, making us sick and unhappy.
AHS is fun and inspiring, and you’ll leave having made new friends and with new ideas about how to optimize your health
If you decide to join us, please come say hello. Tickets are available through the AHS Website, at ancestralhealth.org — [“Ancestral Health Dot Org”] — where you can also see the three-day schedule for the event, from August 18 to 20.
You can get a 10% discount using the the Eventbrite promo code “PresenterFriend”.
I just viewed an excellent video presentation from the Institute of Functional Medicine providing very useful data on COVID, particularly focusing on the Omicron variants. You can watch it here:
I will summarize the information. But first a few disclaimers.
I have not vetted all of these notes but none disagree with any reports or studies I have read
I have read many but not all of the studies that support these statements
I viewed the video with frequent pauses and replays to facilitate accurate note taking. If you view the video and find any errors please make a comment.
I had a mild case of breakthrough COVID last week and seem to have some brain-fog, feeling like the morning after working most of the night on-call in the operating room.
Many general observations on varied topics related to COVID-19
Omicron Timeline:
11/11/21 Omicron first appears,
1/15/22 Omicron is 99.5% of US cases
1/26/22 B.2 variant appears in US and Europe
2/5/22 B.2 variant 3.6% of US cases
Omicron presents with about 50 mutations, 15 on the RBD (receptor binding domain) with increased affinity for the ACE 2 receptor
Omicron has a cluster of mutations at the S1S2 Furin Cleavage Site. Furin is an enzyme that cleaves the virus to allow for entry into human cells, present in large amounts in the brain, lung and GI tract (thus omicron affecting these organs perhaps more and possibly increasing the risk in people with comorbidities “associated with Furin”.)
Some Omicron mutations are associated with a degree of immune escape, evading anti-bodies and T cells.
B2 may not be picked up by some tests (not discussed in detail)
Compared to B1, B2 is 2.5 times more transmissible in non-VAX folks.
But Vaccine effectiveness against B2 appears to be at least as good or possibly better than effectiveness against B1. (Strange but stated)
Omicron has on average a 3 day latency between infection and symptoms. It appears to replicate “70X more quickly” compared to delta with 3.5 times greater household transmission. Fortunately lung involvement is 10 times lower compared to the original “Wuhan virus”.
Prior infection with delta DOES NOT SEEM TO PROTECT AGAINST OMICRON.
Hospitalization rate with omicron 38/1000 infections vs 101/1000 infections with delta.
In hospital mortality 29% with delta vs 3% with Omicron BUT because of a dramatic increase in transmission with Omicron, daily death rate in US has been 2200 to 2900 per day during the surge, more than delta. (Greater number of infections outweighs the lower mortality rate)
A preprint study published last month looked at data from about 52,000 people infected with the omicron variant, and about 17,000 infected with delta, in southern California. Compared with patients who had the delta variant, omicron patients had a 53% reduced risk of hospitalization, a 74% reduced risk of ICU admission and a 91% reduced risk of death. The study has not yet been peer-reviewed.
Duration of infection averages 10 days. Estimates for being contagious after onset of symptoms:
5 days 1/3, 7 days 16%, 10 days 5%, therefor some practitioners are recommending isolation for 14 days after onset of symptoms.
PCR can remain positive for months after infection because of non-infectious remnants of viral RNA.
Negative antigen test after isolation is reassuring but does not guarantee patient is not contagious. The home antigen tests were not designed or studied for predicting degree of contagion, only for diagnosis.
LONG COVID can be as high as 30% of all cases, as high as 10% after mild cases.
Vaccination reduces risk of LONG COVID by about 50%.
A study published in GUT demonstrates altered GI microbiome 6 months after infection. The gut microbiome is extremely important for immune function.
One year following COVID infection (previous variants) there is a 60-70% increased risk of heart attack, stroke and congestive heart failure.
In the UK 25% of worker absenteeism is due to LONG COVID.
A Swiss study showed 98% reduction in death with VAX plus booster.
2/15/22 published study from IOWA showed that 90 minutes of exercise on the day of vaccination increased antibody levels measured 4 weeks after vaccination. Similar data are available for influenza vaccination. I reviewed data on various non COVID vaccine effectiveness relative to sleep and exercise in 2 talks given last year. This result is not surprising.
Individuals with infection from prior variants, but not vaccinated, show no effective neutralizing antibody activity against omicron. (Very worrisome, I will try to vet this one)
Omicron has 4.5 times higher re-infection rate compared to delta.
Omicron infection appears to decrease risk of infection with delta, but prior infection with delta (without vaccination) does not appear to protect against omicron.
Prior infection (before omicron) PLUS vaccination provides 76% protection against omicron infection which is about the same protection of VAX + booster, and this appears to include protection against B2 variant.
T cell immunity after infection (pre omicron) and after vaccination appears to persist and T cell activity increases with time after infection and after vaccination.
Novavax has applied for EUA with the FDA. This is a vaccine made with S-protein particles plus adjuvant (no mRNA).
“The Novavax COVID-19 vaccine, codenamed NVX-CoV2373, is a subunit COVID-19 vaccine candidate developed by Novavax and the Coalition for Epidemic Preparedness Innovations (CEPI), brand name Covovax.”
“Results from a Phase 3 clinical trial enrolling 29,960 adult volunteers in the United States and Mexico show that the investigational vaccine known as NVX-CoV2373 demonstrated 90.4% efficacy in preventing symptomatic COVID-19 disease. The candidate showed 100% protection against moderate and severe disease. In people at high risk of developing complications from COVID-19 (people 65 years or older and people under age 65 with certain comorbidities or with likely regular exposure to COVID-19), the vaccine showed 91.0% efficacy in preventing symptomatic COVID-19 disease.”
The US Army is in phase I clinical trial with a multi-valent “ferritin nanoparticle multi-faced” vaccine. This “soccer ball shaped” vaccine has 24 “faces” with multiple variant antigens. Each “face” carries a different antigen.
“The Spike Ferritin Nanoparticle platform is designed to protect against an array of SARS-CoV-2 variants and SARS-origin variants but was not tested on the Omicron variant,” Walter Reed officials said.
J&J vaccine issues:
The J&J vaccine is associated with a risk of thrombosis-thrombocytopenia (blood clots and decreased platelets). Risk: 1:100,000 doses in women age 30-50. CDC recommends against J&J vaccine unless there is a contra-indication to mRNA vaccine. 15% of these cases are fatal.
A full discussion of therapeutics (drugs) against COVID can be read at IFM.org/COVID
PAXLOVID is an oral combination of two anti-viral medications reserved for adults (age >= 18) with increased risk, given within day 3-5 of symptom onset. It decreases risk of hospitalization and death by about 70% in low-risk and 89% in high risk groups. There are many contra-indications to use including specific medications and supplements (such as Saint John’s Wort). Availability is a problem.
A recent study published in NEJM used IV Remdesivir (daily for 3 days) for early out- patient treatment in high risk patients, reduced risk of hospitalization/death by 87%. This would represent an off-label use of the drug based on a well controlled study.
Home antigen tests on average become positive 3 days after first positive PCR (nasal swab), 2 days after a positive saliva PCR.
The BiaxNOW home antigen test is 73% sensitive (27% false negative rate)
Pregnancy-COVID and vaccination:
A study of 40,000 pregnant women found no increase in pre-term birth, small for gestational age, or any other complication following vaccination during pregnancy.
But COVID infection in unvaccinated women during pregnancy is associated with increased risk for pre-term birth, still born, low birth weight, cesarean section, decreased fetal growth, maternal intubation and death.
Maternal Vaccination produces anti-Covid antibodies found in fetal cord blood at birth.
Intra-uterine demise with COVID is associated with massive placental insufficiency.
There is no data to support decreased female or male fertility following vaccination.
A study of menstrual regularity following vaccination showed < 1 day change in cycle length post vaccination, not clinically significant. Post vaccination regularity equivalent to expected variation in menstrual cycles.
Two months following COVID infection there is a decrease in male but not female fertility rate.
Multiple studies have demonstrated association between low Vitamin D status and risk for severe-critical disease and death. Association does not equal causation but there is biologic plausibility (Vitamin D is a major immune regulator) and consistently increased risk associated with low levels. A recent study demonstrated 14 times greater risk for severe-critical disease in hospitalized patients with levels <20 compared to patients with levels >40. I will update my previous discussion of Vitamin D and COVID in a future post. Spoiler alert: An intervention study with high dose Vitamin D done in Spain demonstrated improved clinical outcome.
Risk factors for poor outcome in descending order:
Age > 65
immuno-compromised state
lung disease
liver disease
kidney disease
neurologic disorders
diabetes
cardiac disease
Patients with severe disease had >= 1 risk factor
78% of patients who died had >= 4 risk factors.
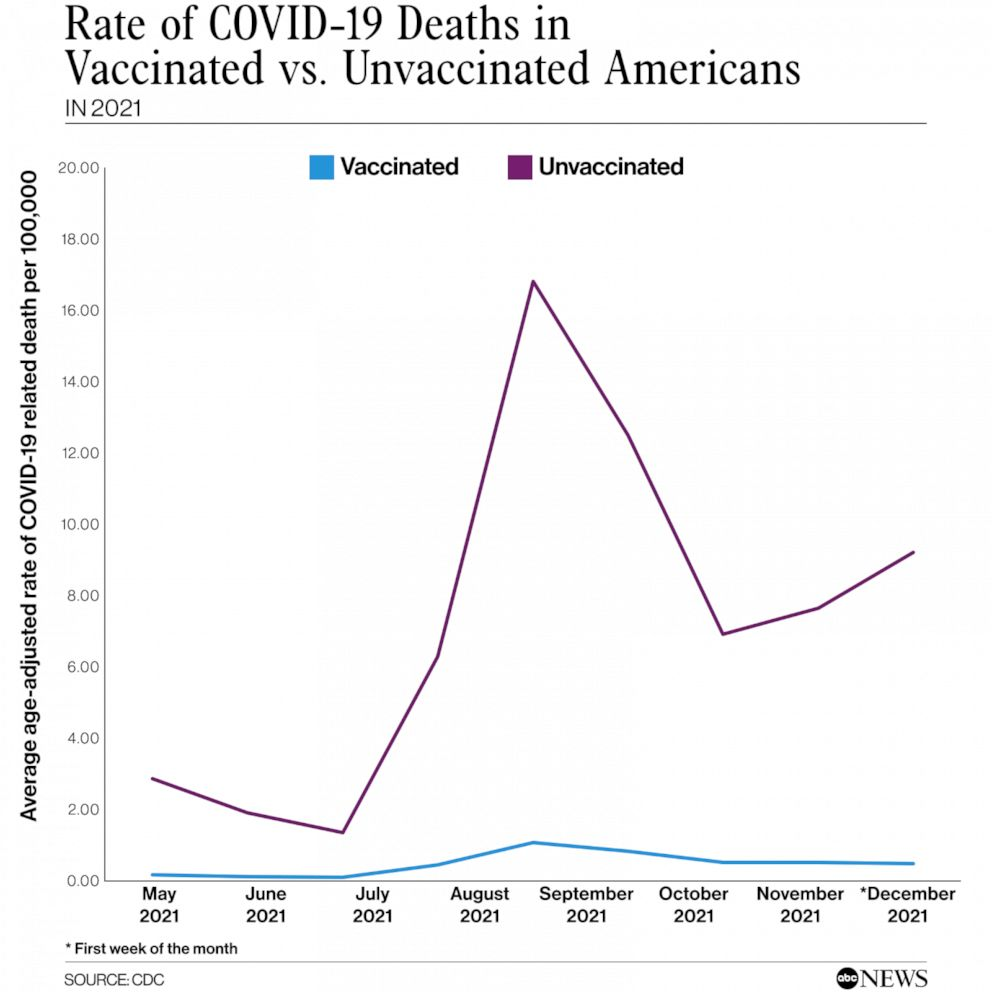
“Nearly two years into the pandemic, unvaccinated Americans are still making up the majority of COVID deaths.”
“Data from the Centers for Disease Control and Prevention shows that during the first week of December — when the omicron variant began taking hold — unvaccinated people were dying at a rate of 9 per 100,000.”
“By comparison, fully vaccinated people were dying at a rate of 0.4 per 100,000, meaning unvaccinated people were 20 times more likely to die of the virus”
In the context of the COVID 19 pandemic I will close with the usual summary.
Exercise, especially out of doors in a green space, supports the immune system
Get some sunshine and make sure you have adequate Vitamin D levels. Supplement with Vitamin D3 to get your levels above 30 ng/ml, >40ng/ml arguably better.
Eliminate sugar-added foods and beverages from your diet. These increase inflammation, cause metabolic dysfunction, and suppress immunity.
Eliminate refined-inflammatory “vegetable oils” from your diet, instead eat healthy fat.
Clean up your home environment and minimize your family’s exposure to environmental toxins by following recommendations at EWG.org with regards to household products, personal care products, and organic foods. (https://www.ewg.org/)
Drink water filtered through a high quality system that eliminates most environmental toxins.
If you are eligible for vaccination, consider protecting yourself and your neighbor with a few jabs. Age > 50 and/or risk factors means clear benefit from a booster.
THIS WEBSITE PROVIDES INFORMATION FOR EDUCATIONAL PURPOSES ONLY. CONSULT YOUR HEALTH CARE PROVIDER FOR MEDICAL ADVICE.
Eat clean, drink filtered water, love, laugh, exercise outdoors in a greenspace, get some morning sunlight, block the blue light before bed, engage in meaningful work, find a sense of purpose, spend time with those you love, AND sleep well tonight.
Today I listened to Dr. Bruce Patterson discuss his research on Long-Covid.
Bruce Patterson was director of a virology lab at Stanford before establishing Incelldx, a biotech firm in the area of virus diagnostics. Bruce was interviewed today (second half of the program) on The People’s Pharmacy (NPR). The transcript and podcast will be available tomorrow at PeoplesPharmacy.com (show #1273)
Utilizing AI and data from over 10,000 patients, Incelldx has developed diagnostic tools to characterize the immune system dysregulation associated with long covid. According to Dr. Patterson’s research, Long-Covid involves “non-classical monocytes” that are reacting to remnant virus proteins (not RNA or DNA), producing a vascular inflammatory process. That was the missing link. Researchers were looking for RNA, but the problem appears to be in the monocyte reaction to remnant viral proteins that stimulate these specialized monocytes, producing a chronic vasculitis.
Here is a link to the Long Covid clinical program based upon this research.
The program involves immune testing by Incelldx and based on the results, treatment recommendations are made.
So far 2 drugs repurposed for long-Covid appear effective when used in combination.
A CCR5 antagonist (maraviroc) which has been used to treat HIV and a Statin medication which blocks binding of the monocytes to artery walls.
According to Dr. Patterson, Long Covid in many patients is a vascular inflammatory process, mediated by non-classical monocytes which are activated by viral remnant proteins.
Dr. Patterson has seen many patients respond to this drug combination. He uses an old, early statin drug (pravastatin) which has a low side effect profile compared to the more commonly used atorvastatin (which gave me severe myopathy, notorious for that problem but understated by drug company reports).
This is cutting edge, most physicians, even in university settings, are not aware of this diagnostic/therapeutic approach.
This is still considered experimental but appears to be very promising.
In the context of the COVID 19 pandemic I will close with the usual summary.
Exercise, especially out of doors in a green space, supports the immune system
Get some sunshine and make sure you have adequate Vitamin D levels. Supplement with Vitamin D3 to get your levels above 30 ng/ml. (read this Open Letter)
Eliminate sugar-added foods and beverages from your diet. These increase inflammation, cause metabolic dysfunction, and suppress immunity.
Eliminate refined-inflammatory “vegetable oils” from your diet, instead eat healthy fat.
Clean up your home environment and minimize your family’s exposure to environmental toxins by following recommendations at EWG.org with regards to household products, personal care products, and organic foods. (https://www.ewg.org/)
If you are over age 12 and eligible for vaccination, consider protecting yourself and your neighbor with vaccination.
THIS WEBSITE PROVIDES INFORMATION FOR EDUCATIONAL PURPOSES ONLY. CONSULT YOUR HEALTH CARE PROVIDER FOR MEDICAL ADVICE.
Eat clean, drink filtered water, love, laugh, exercise outdoors in a greenspace, get some morning sunlight, block the blue light before bed, engage in meaningful work, find a sense of purpose, spend time with those you love, AND sleep well tonight.
A recently published study from Israel compared vaccinated vs unvaccinated people who developed COVID 19. The study was huge. It evaluated the absolute risk of various events following vaccination vs no vaccination with COVID-19 infection. The absolute risk numbers are presented as # of events per 100,000 people. The data clearly shows safety of the vaccine and a large difference between vaccination vs no vaccination/infection. The study matched vaccinated individuals with unvaccinated individuals (before the vaccine was available) for various risk factors and followed the two groups for 42 days. Events were recorded during the 42-day study period.
Here is a summary of the findings. The vaccine was the mRNA vaccine (Pfizer).
“We used a data set involving more than 2.4 million vaccinated persons from an integrated health care organization to evaluate the safety profile of the BNT162b2 mRNA Covid-19 vaccine. The main potential adverse events identified included an excess risk of lymphadenopathy (78.4 events per 100,000 persons), herpes zoster infection (15.8 events), appendicitis (5.0 events), and myocarditis (2.7 events).
To place these risks in context, we also examined data on more than 240,000 infected persons to estimate the effects of a documented SARS-CoV-2 infection on the incidence of the same adverse events. SARS-CoV-2 infection was not estimated to have a meaningful effect on the incidence of lymphadenopathy, herpes zoster infection, or appendicitis, but it was estimated to result in a substantial excess risk of myocarditis (11.0 events per 100,000 persons). SARS-CoV-2 infection was also estimated to substantially increase the risk of several adverse events for which vaccination was not found to increase the risk, including an estimated excess risk of arrhythmia (166.1 events per 100,000 persons), acute kidney injury (125.4 events), pulmonary embolism (61.7 events), deep-vein thrombosis (43.0 events), myocardial infarction (25.1 events), pericarditis (10.9 events), and intracranial hemorrhage (7.6 events).
Another particularly notable class of adverse events that has been reported in the context of Covid-19 vaccines is thromboembolic events. These adverse events, which primarily affect young women, have been linked with the ChAdOx1 nCoV-1932 and Ad26.COV2.S (Johnson & Johnson–Janssen) Covid-19 vaccines,33 both of which are adenoviral vector vaccines. However, we did not find an association between the BNT162b2 (mRNA) vaccine and various thromboembolic events in this study.”
We already know that vaccination substantially decreases the risk of severe illness, hospitalization and death. The media has reported on potential, rare complications of the vaccine. Those reports have frightened some people primarily because when the media report them in a sensational way, they do not compare the risk of the same events with infection. This study demonstrates that the rare complications of vaccination pale in comparison to the risk of the same complications with infection. This study also identifies several serious complications of infection that do not occur as a result of vaccination.
Exercise, especially out of doors in a green space, supports the immune system
Get some sunshine and make sure you have adequate Vitamin D levels. Supplement with Vitamin D3 to get your levels above 30 ng/ml. (read this Open Letter)
Eliminate sugar-added foods and beverages from your diet. These increase inflammation, cause metabolic dysfunction, and suppress immunity.
Eliminate refined-inflammatory “vegetable oils” from your diet, instead eat healthy fat.
Clean up your home environment and minimize your family’s exposure to environmental toxins by following recommendations at EWG.org with regards to household products, personal care products, and organic foods. (https://www.ewg.org/)
If you are over age 12 and eligible for vaccination, consider protecting yourself and your neighbor with vaccination.
THIS WEBSITE PROVIDES INFORMATION FOR EDUCATIONAL PURPOSES ONLY. CONSULT YOUR HEALTH CARE PROVIDER FOR MEDICAL ADVICE.
Eat clean, drink filtered water, love, laugh, exercise outdoors in a greenspace, get some morning sunlight, block the blue light before bed, engage in meaningful work, find a sense of purpose, spend time with those you love, AND sleep well tonight.