I recently gave a talk at the AHS 2022 meeting held at UCLA. You can view the video here:
This first slide gives a good overview.
The presentation covers a quick review of my presentations given last year at the PAH 2021 annual meeting (virtual) with additional information on long Covid.
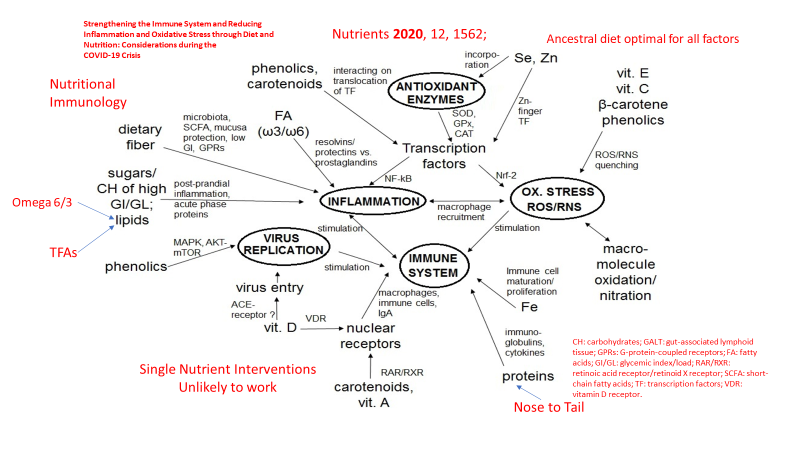
Multiple nutrients acting synergistically support a balanced response to viral infections, including SARS CoV-2. Here is a picture.
The take home message is that no single nutritional intervention is likely to have significant impact with an acute infection unless all but one nutritional component is optimal. Nevertheless, there is compelling evidence that Vitamin D deficiency is rampant in the developed world and if one nutritional intervention is likely to be of benefit, Vitamin D supplementation, particularly in high risk populations, presents the most likely candidate. As usual, preventive supplementation would be preferable to rescue high dose intervention.
In a study of frail elderly hospitalized patients, regular vitamin D supplementation was associated with decreased mortality as demonstrated here. Compared to no supplementation, regular supplementation was associated with a 93% reduction in risk of death.
A study from Spain with very high dose Vitamin D in the form of Calcifediol showed significant benefit in hospitalized patients, suggesting that Vitamin D deficiency was prevalent in that population and that such a treatment intervention should be widely considered.
Calcifediol Treatment and COVID-19-Related Outcomes
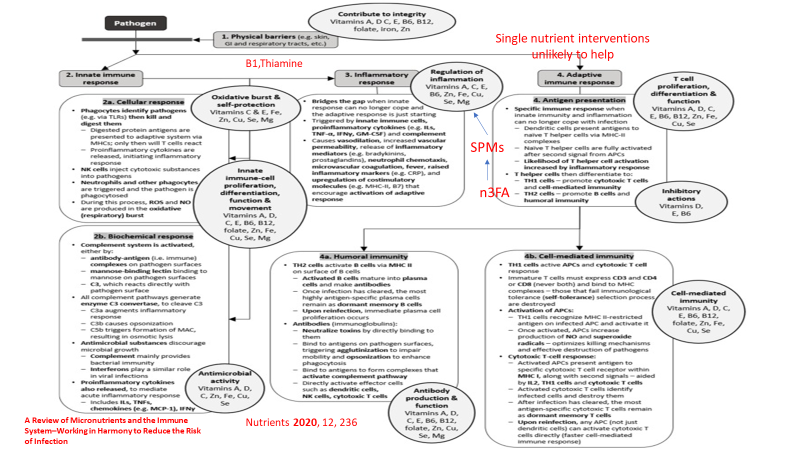
The following graphic from another nutrition review article, with red additions added by myself, demonstrates the complex interaction between nutrition and the two main components of our immune system, innate immunity (immediate response) and adaptive immunity (based on immune memory). Again red highlights added by yours truely.
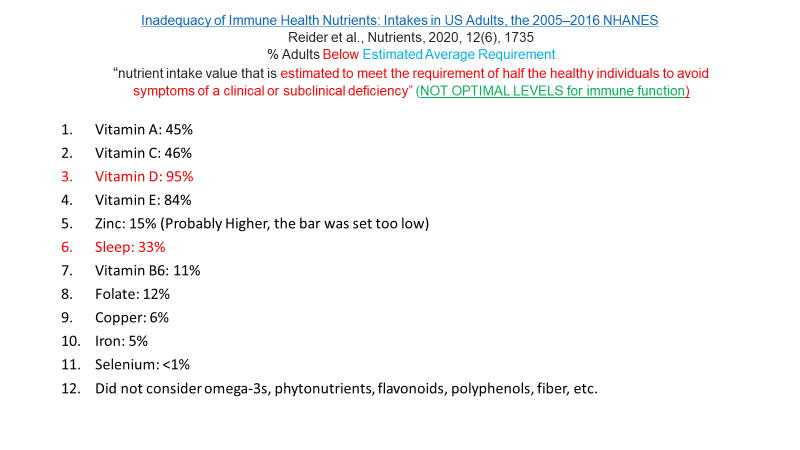
And here is a slide from my lecture with quotes from that article.
Yet most Americans are deficient in many of these essential nutrients as depicted here. The percentages represent the % of Americans that fall below the estimated amount required to prevent deficiency in HALF of adults (a very low standard).
The EAR is a very low bar to meet, yet many Americans fall below even that low standard.
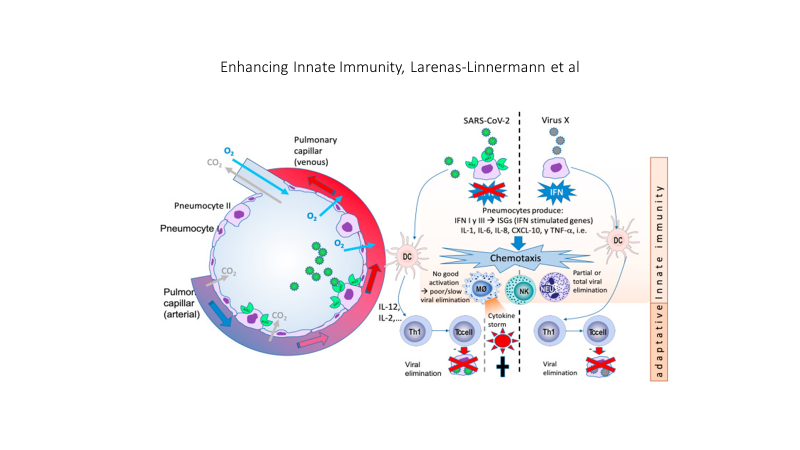
The SARS CoV2 virus interferes with a crucial component of the the initial (innate) immune response, the production of interferon 1 and the signaling of interferon one to immune cell mediators as depicted in this graphic.
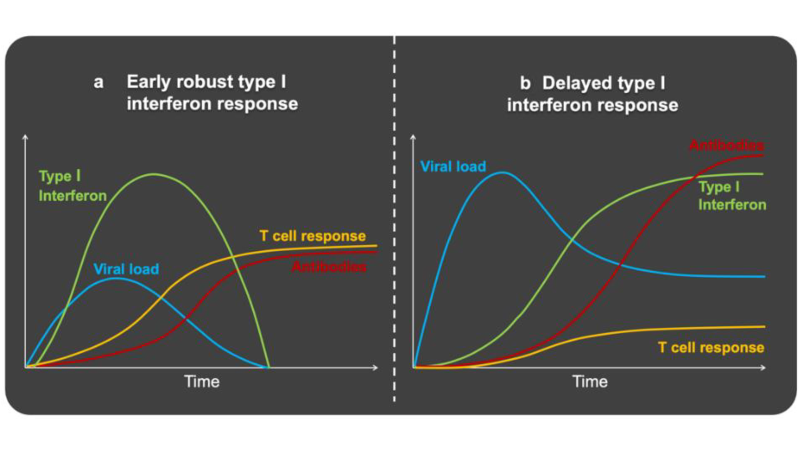
SARS CoV2 on the left is compared to Virus X on the right. On the left interferon 1 (IFN) production and signaling is blocked by the virus, interfering with an effective and controlled immune response, on the right IFN is not blocked. A cascade of events results in TOO LITTLE, TOO LATE, AND THEN TOO MUCH of an immune response, producing a cytokine storm.
Obesity, insulin and leptin resistance, also interfere with the production and signaling of interferon. The result is that people with insulin and leptin resistance (pre-diabetes, Type 2 Diabetes as well as sarcopenia) experience a double hit. First the virus itself disrupts the immune response and superimposed upon the viral effect is the effect of insulin and leptin resistance on the immune response.
SOCS: suppressor of cytokine signaling. Several recent viral studies have shown that viral genes can hijack SOCS1 to inhibit host antiviral pathways, as a strategy to evade host immunityOn the left Interferon production and signaling are normal and a successful immune response is mounted. On the right the presence of insulin and leptin resistance, associated with obesity results in an initial inadequate response and a late excessive response. TOO LITTLE, TOO LATE, THEN TOO MUCH.
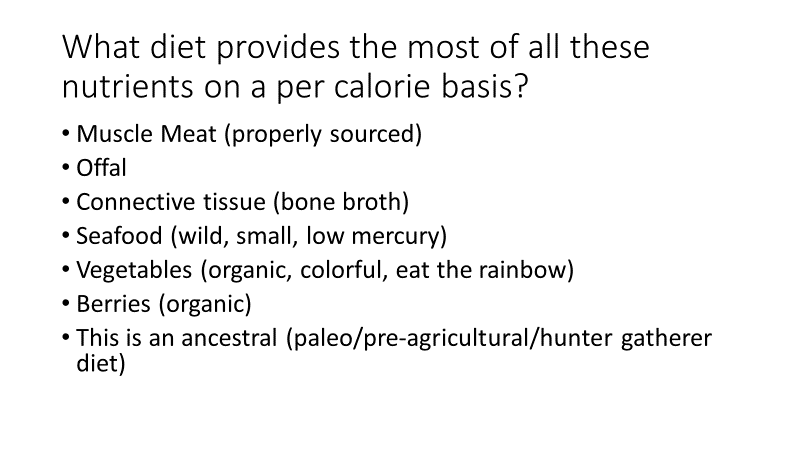
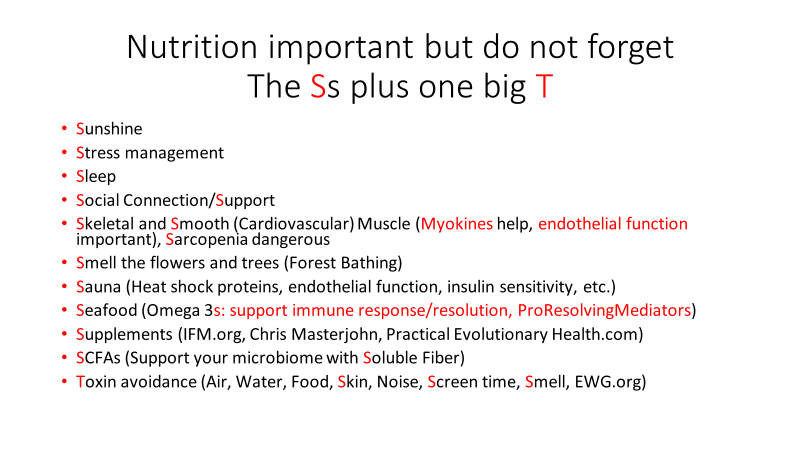
Factors that can quickly impact insulin and leptin resistance include all the components of an ancestral lifestyle depicted in my website graphic. A paleolithic or ancestral diet that eliminates sugar added foods and beverages, replacing those empty calories with nutrient dense foods, exercise, adequate restorative sleep, stress reduction, avoidance of environmental toxins, social connection. All of these affect health in general, mitigate insulin and leptin resistance, and support a balanced immune response to viral infection. The circle of health depicted below is surrounded by the many deleterious aspects of modern living. Thus, a mismatch between our evolutionary biology and present day life.
Here is a slide from my lecture that lists many lifestyle factors that can impact infection with any virus, including SARS CoV-2
My lecture also included discussion of Long COVID, theories of etiology and pathophysiology which will be discussed in my next post.
For the full lecture which is about 34 minutes long, please follow the link above.
THIS WEBSITE PROVIDES INFORMATION FOR EDUCATIONAL PURPOSES ONLY. CONSULT YOUR HEALTH CARE PROVIDER FOR MEDICAL ADVICE.
Eat clean, drink filtered water, love, laugh, exercise outdoors in a greenspace, get some morning sunlight, block the blue light before bed, engage in meaningful work, find a sense of purpose, spend time with those you love, AND sleep well tonight.
I just viewed an excellent video presentation from the Institute of Functional Medicine providing very useful data on COVID, particularly focusing on the Omicron variants. You can watch it here:
I will summarize the information. But first a few disclaimers.
I have not vetted all of these notes but none disagree with any reports or studies I have read
I have read many but not all of the studies that support these statements
I viewed the video with frequent pauses and replays to facilitate accurate note taking. If you view the video and find any errors please make a comment.
I had a mild case of breakthrough COVID last week and seem to have some brain-fog, feeling like the morning after working most of the night on-call in the operating room.
Many general observations on varied topics related to COVID-19
Omicron Timeline:
11/11/21 Omicron first appears,
1/15/22 Omicron is 99.5% of US cases
1/26/22 B.2 variant appears in US and Europe
2/5/22 B.2 variant 3.6% of US cases
Omicron presents with about 50 mutations, 15 on the RBD (receptor binding domain) with increased affinity for the ACE 2 receptor
Omicron has a cluster of mutations at the S1S2 Furin Cleavage Site. Furin is an enzyme that cleaves the virus to allow for entry into human cells, present in large amounts in the brain, lung and GI tract (thus omicron affecting these organs perhaps more and possibly increasing the risk in people with comorbidities “associated with Furin”.)
Some Omicron mutations are associated with a degree of immune escape, evading anti-bodies and T cells.
B2 may not be picked up by some tests (not discussed in detail)
Compared to B1, B2 is 2.5 times more transmissible in non-VAX folks.
But Vaccine effectiveness against B2 appears to be at least as good or possibly better than effectiveness against B1. (Strange but stated)
Omicron has on average a 3 day latency between infection and symptoms. It appears to replicate “70X more quickly” compared to delta with 3.5 times greater household transmission. Fortunately lung involvement is 10 times lower compared to the original “Wuhan virus”.
Prior infection with delta DOES NOT SEEM TO PROTECT AGAINST OMICRON.
Hospitalization rate with omicron 38/1000 infections vs 101/1000 infections with delta.
In hospital mortality 29% with delta vs 3% with Omicron BUT because of a dramatic increase in transmission with Omicron, daily death rate in US has been 2200 to 2900 per day during the surge, more than delta. (Greater number of infections outweighs the lower mortality rate)
A preprint study published last month looked at data from about 52,000 people infected with the omicron variant, and about 17,000 infected with delta, in southern California. Compared with patients who had the delta variant, omicron patients had a 53% reduced risk of hospitalization, a 74% reduced risk of ICU admission and a 91% reduced risk of death. The study has not yet been peer-reviewed.
Duration of infection averages 10 days. Estimates for being contagious after onset of symptoms:
5 days 1/3, 7 days 16%, 10 days 5%, therefor some practitioners are recommending isolation for 14 days after onset of symptoms.
PCR can remain positive for months after infection because of non-infectious remnants of viral RNA.
Negative antigen test after isolation is reassuring but does not guarantee patient is not contagious. The home antigen tests were not designed or studied for predicting degree of contagion, only for diagnosis.
LONG COVID can be as high as 30% of all cases, as high as 10% after mild cases.
Vaccination reduces risk of LONG COVID by about 50%.
A study published in GUT demonstrates altered GI microbiome 6 months after infection. The gut microbiome is extremely important for immune function.
One year following COVID infection (previous variants) there is a 60-70% increased risk of heart attack, stroke and congestive heart failure.
In the UK 25% of worker absenteeism is due to LONG COVID.
A Swiss study showed 98% reduction in death with VAX plus booster.
2/15/22 published study from IOWA showed that 90 minutes of exercise on the day of vaccination increased antibody levels measured 4 weeks after vaccination. Similar data are available for influenza vaccination. I reviewed data on various non COVID vaccine effectiveness relative to sleep and exercise in 2 talks given last year. This result is not surprising.
Individuals with infection from prior variants, but not vaccinated, show no effective neutralizing antibody activity against omicron. (Very worrisome, I will try to vet this one)
Omicron has 4.5 times higher re-infection rate compared to delta.
Omicron infection appears to decrease risk of infection with delta, but prior infection with delta (without vaccination) does not appear to protect against omicron.
Prior infection (before omicron) PLUS vaccination provides 76% protection against omicron infection which is about the same protection of VAX + booster, and this appears to include protection against B2 variant.
T cell immunity after infection (pre omicron) and after vaccination appears to persist and T cell activity increases with time after infection and after vaccination.
Novavax has applied for EUA with the FDA. This is a vaccine made with S-protein particles plus adjuvant (no mRNA).
“The Novavax COVID-19 vaccine, codenamed NVX-CoV2373, is a subunit COVID-19 vaccine candidate developed by Novavax and the Coalition for Epidemic Preparedness Innovations (CEPI), brand name Covovax.”
“Results from a Phase 3 clinical trial enrolling 29,960 adult volunteers in the United States and Mexico show that the investigational vaccine known as NVX-CoV2373 demonstrated 90.4% efficacy in preventing symptomatic COVID-19 disease. The candidate showed 100% protection against moderate and severe disease. In people at high risk of developing complications from COVID-19 (people 65 years or older and people under age 65 with certain comorbidities or with likely regular exposure to COVID-19), the vaccine showed 91.0% efficacy in preventing symptomatic COVID-19 disease.”
The US Army is in phase I clinical trial with a multi-valent “ferritin nanoparticle multi-faced” vaccine. This “soccer ball shaped” vaccine has 24 “faces” with multiple variant antigens. Each “face” carries a different antigen.
“The Spike Ferritin Nanoparticle platform is designed to protect against an array of SARS-CoV-2 variants and SARS-origin variants but was not tested on the Omicron variant,” Walter Reed officials said.
J&J vaccine issues:
The J&J vaccine is associated with a risk of thrombosis-thrombocytopenia (blood clots and decreased platelets). Risk: 1:100,000 doses in women age 30-50. CDC recommends against J&J vaccine unless there is a contra-indication to mRNA vaccine. 15% of these cases are fatal.
A full discussion of therapeutics (drugs) against COVID can be read at IFM.org/COVID
PAXLOVID is an oral combination of two anti-viral medications reserved for adults (age >= 18) with increased risk, given within day 3-5 of symptom onset. It decreases risk of hospitalization and death by about 70% in low-risk and 89% in high risk groups. There are many contra-indications to use including specific medications and supplements (such as Saint John’s Wort). Availability is a problem.
A recent study published in NEJM used IV Remdesivir (daily for 3 days) for early out- patient treatment in high risk patients, reduced risk of hospitalization/death by 87%. This would represent an off-label use of the drug based on a well controlled study.
Home antigen tests on average become positive 3 days after first positive PCR (nasal swab), 2 days after a positive saliva PCR.
The BiaxNOW home antigen test is 73% sensitive (27% false negative rate)
Pregnancy-COVID and vaccination:
A study of 40,000 pregnant women found no increase in pre-term birth, small for gestational age, or any other complication following vaccination during pregnancy.
But COVID infection in unvaccinated women during pregnancy is associated with increased risk for pre-term birth, still born, low birth weight, cesarean section, decreased fetal growth, maternal intubation and death.
Maternal Vaccination produces anti-Covid antibodies found in fetal cord blood at birth.
Intra-uterine demise with COVID is associated with massive placental insufficiency.
There is no data to support decreased female or male fertility following vaccination.
A study of menstrual regularity following vaccination showed < 1 day change in cycle length post vaccination, not clinically significant. Post vaccination regularity equivalent to expected variation in menstrual cycles.
Two months following COVID infection there is a decrease in male but not female fertility rate.
Multiple studies have demonstrated association between low Vitamin D status and risk for severe-critical disease and death. Association does not equal causation but there is biologic plausibility (Vitamin D is a major immune regulator) and consistently increased risk associated with low levels. A recent study demonstrated 14 times greater risk for severe-critical disease in hospitalized patients with levels <20 compared to patients with levels >40. I will update my previous discussion of Vitamin D and COVID in a future post. Spoiler alert: An intervention study with high dose Vitamin D done in Spain demonstrated improved clinical outcome.
Risk factors for poor outcome in descending order:
Age > 65
immuno-compromised state
lung disease
liver disease
kidney disease
neurologic disorders
diabetes
cardiac disease
Patients with severe disease had >= 1 risk factor
78% of patients who died had >= 4 risk factors.
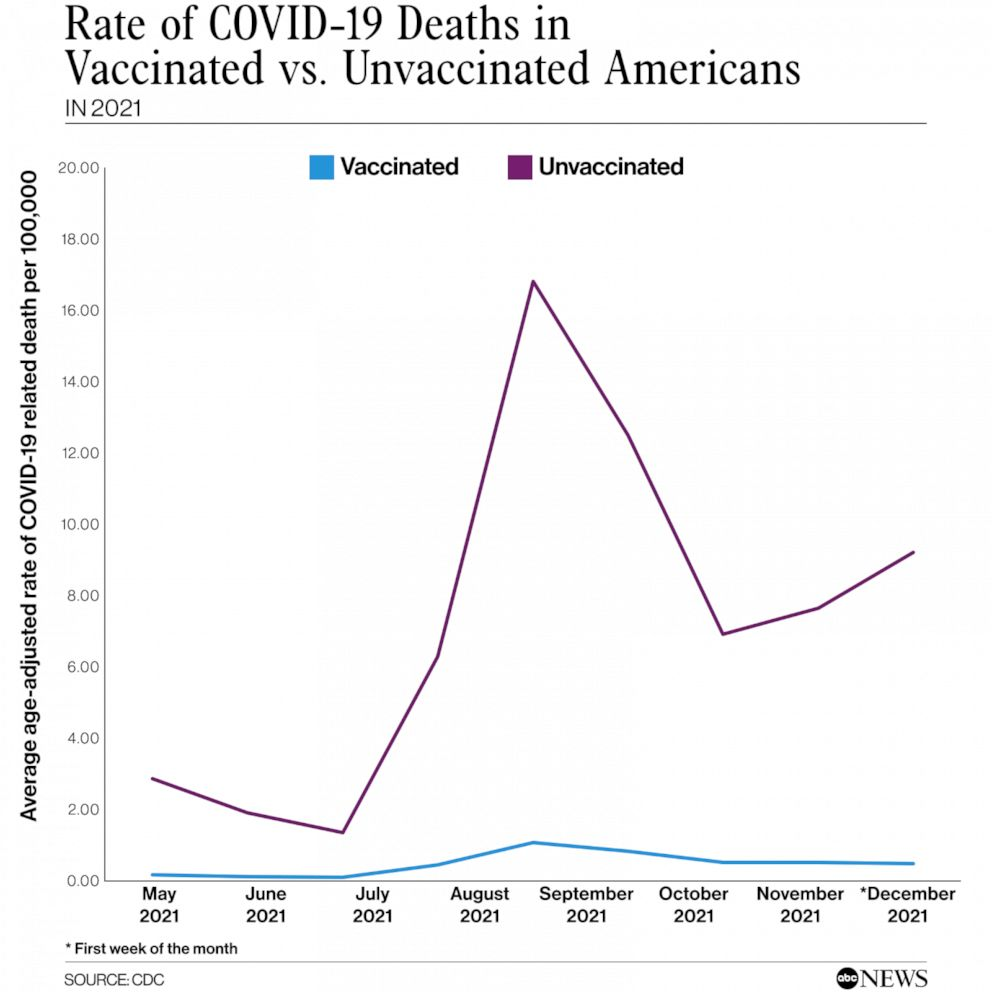
“Nearly two years into the pandemic, unvaccinated Americans are still making up the majority of COVID deaths.”
“Data from the Centers for Disease Control and Prevention shows that during the first week of December — when the omicron variant began taking hold — unvaccinated people were dying at a rate of 9 per 100,000.”
“By comparison, fully vaccinated people were dying at a rate of 0.4 per 100,000, meaning unvaccinated people were 20 times more likely to die of the virus”
In the context of the COVID 19 pandemic I will close with the usual summary.
Exercise, especially out of doors in a green space, supports the immune system
Get some sunshine and make sure you have adequate Vitamin D levels. Supplement with Vitamin D3 to get your levels above 30 ng/ml, >40ng/ml arguably better.
Eliminate sugar-added foods and beverages from your diet. These increase inflammation, cause metabolic dysfunction, and suppress immunity.
Eliminate refined-inflammatory “vegetable oils” from your diet, instead eat healthy fat.
Clean up your home environment and minimize your family’s exposure to environmental toxins by following recommendations at EWG.org with regards to household products, personal care products, and organic foods. (https://www.ewg.org/)
Drink water filtered through a high quality system that eliminates most environmental toxins.
If you are eligible for vaccination, consider protecting yourself and your neighbor with a few jabs. Age > 50 and/or risk factors means clear benefit from a booster.
THIS WEBSITE PROVIDES INFORMATION FOR EDUCATIONAL PURPOSES ONLY. CONSULT YOUR HEALTH CARE PROVIDER FOR MEDICAL ADVICE.
Eat clean, drink filtered water, love, laugh, exercise outdoors in a greenspace, get some morning sunlight, block the blue light before bed, engage in meaningful work, find a sense of purpose, spend time with those you love, AND sleep well tonight.
A recently published study from Israel compared vaccinated vs unvaccinated people who developed COVID 19. The study was huge. It evaluated the absolute risk of various events following vaccination vs no vaccination with COVID-19 infection. The absolute risk numbers are presented as # of events per 100,000 people. The data clearly shows safety of the vaccine and a large difference between vaccination vs no vaccination/infection. The study matched vaccinated individuals with unvaccinated individuals (before the vaccine was available) for various risk factors and followed the two groups for 42 days. Events were recorded during the 42-day study period.
Here is a summary of the findings. The vaccine was the mRNA vaccine (Pfizer).
“We used a data set involving more than 2.4 million vaccinated persons from an integrated health care organization to evaluate the safety profile of the BNT162b2 mRNA Covid-19 vaccine. The main potential adverse events identified included an excess risk of lymphadenopathy (78.4 events per 100,000 persons), herpes zoster infection (15.8 events), appendicitis (5.0 events), and myocarditis (2.7 events).
To place these risks in context, we also examined data on more than 240,000 infected persons to estimate the effects of a documented SARS-CoV-2 infection on the incidence of the same adverse events. SARS-CoV-2 infection was not estimated to have a meaningful effect on the incidence of lymphadenopathy, herpes zoster infection, or appendicitis, but it was estimated to result in a substantial excess risk of myocarditis (11.0 events per 100,000 persons). SARS-CoV-2 infection was also estimated to substantially increase the risk of several adverse events for which vaccination was not found to increase the risk, including an estimated excess risk of arrhythmia (166.1 events per 100,000 persons), acute kidney injury (125.4 events), pulmonary embolism (61.7 events), deep-vein thrombosis (43.0 events), myocardial infarction (25.1 events), pericarditis (10.9 events), and intracranial hemorrhage (7.6 events).
Another particularly notable class of adverse events that has been reported in the context of Covid-19 vaccines is thromboembolic events. These adverse events, which primarily affect young women, have been linked with the ChAdOx1 nCoV-1932 and Ad26.COV2.S (Johnson & Johnson–Janssen) Covid-19 vaccines,33 both of which are adenoviral vector vaccines. However, we did not find an association between the BNT162b2 (mRNA) vaccine and various thromboembolic events in this study.”
We already know that vaccination substantially decreases the risk of severe illness, hospitalization and death. The media has reported on potential, rare complications of the vaccine. Those reports have frightened some people primarily because when the media report them in a sensational way, they do not compare the risk of the same events with infection. This study demonstrates that the rare complications of vaccination pale in comparison to the risk of the same complications with infection. This study also identifies several serious complications of infection that do not occur as a result of vaccination.
Exercise, especially out of doors in a green space, supports the immune system
Get some sunshine and make sure you have adequate Vitamin D levels. Supplement with Vitamin D3 to get your levels above 30 ng/ml. (read this Open Letter)
Eliminate sugar-added foods and beverages from your diet. These increase inflammation, cause metabolic dysfunction, and suppress immunity.
Eliminate refined-inflammatory “vegetable oils” from your diet, instead eat healthy fat.
Clean up your home environment and minimize your family’s exposure to environmental toxins by following recommendations at EWG.org with regards to household products, personal care products, and organic foods. (https://www.ewg.org/)
If you are over age 12 and eligible for vaccination, consider protecting yourself and your neighbor with vaccination.
THIS WEBSITE PROVIDES INFORMATION FOR EDUCATIONAL PURPOSES ONLY. CONSULT YOUR HEALTH CARE PROVIDER FOR MEDICAL ADVICE.
Eat clean, drink filtered water, love, laugh, exercise outdoors in a greenspace, get some morning sunlight, block the blue light before bed, engage in meaningful work, find a sense of purpose, spend time with those you love, AND sleep well tonight.
I just read an article by an immunocompromised physician published in JAMA (Journal of the American Medical Association). In this article, Dr. Lindsay Ryan, an ER physician who takes immunosuppressive medication to treat her auto-immune disease, describes her thoughts on folks who refuse to be vaccinated against COVID-19. She acknowledges the many possible reasons one might choose to avoid vaccination, many related to lack of scientific information and confusion by false information so widely spread on the internet. At the heart of her discussion lays a fundamental conflict, individual freedom vs responsibility to protect our neighbor. Dr. Ryan has been vaccinated but her immunosuppressant medication has significantly blunted her response to vaccination, leaving her unprotected by the vaccine. Therefore in her job as an ER physician she is constantly at risk for infection from an asymptomatic or symptomatic patient with any infectious disease including COVID-19. Beyond that, living a “normal life” will remain elusive for her as so many individuals continue to refuse vaccination based on a “freedom of choice” decision which places their own freedom over the interests of one’s neighbor. Many Americans are immuno-compromised. There are many medications that render the immune system less effective to various degrees. There are many conditions that compromise immune systems and render vaccination less effective. By definition, all patients who have received an organ transplant are immunocompromised. All such individuals are at increased risk of death or disability from COVID-19 exposure. The single most effective way to help protect these individuals is for everyone eligible to become vaccinated.
You can learn more about organ transplants by perusing organ transplant data for the USA. Your neighbor, the person you pass in the aisle of the grocery store, the person who is sitting in the restaurant at a table next to you, could be a transplant recipient or on an immunosuppressive drug for auto-immune disease.
According to the National Institutes of Health, up to 23.5 million Americans (more than seven percent of the population) suffer from an autoimmune disease—and the prevalence is rising.
Alternatively, they may be immunosuppressed because of chemotherapy for cancer.
How many people in the United States have cancer? More than 16.9 million Americans (8.1 million males and 8.8 million females) with a history of cancer were alive on January 1, 2019; this number is projected to reach more than 22.1 million by January 1, 2030 based on the growth and aging of the population alone.
If you choose to avoid vaccination as a form of personal freedom expression, is that choice a charitable or responsible choice? Does it balance personal freedom against responsibility for the health and safety of our neighbor? Are not immuno-compromised individuals entitled to “life, liberty and pursuit of happiness” and freedom from unnecessary risk exposure because of their neighbor’s personal choices?
We have laws against driving under the influence. Such laws seek a balance between personal freedom and responsibility towards one’s neighbor. As a society we have accepted restrictions on personal behavior that places others at risk and we have instituted laws to enforce such restrictions.
In the context of the COVID 19 pandemic I will close with the usual summary.
Exercise, especially out of doors in a green space, supports the immune system
Get some sunshine and make sure you have adequate Vitamin D levels. Supplement with Vitamin D3 to get your levels above 30 ng/ml. (read this Open Letter)
Eliminate sugar-added foods and beverages from your diet. These increase inflammation, cause metabolic dysfunction, and suppress immunity.
Eliminate refined-inflammatory “vegetable oils” from your diet, instead eat healthy fat.
Clean up your home environment and minimize your family’s exposure to environmental toxins by following recommendations at EWG.org with regards to household products, personal care products, and organic foods. (https://www.ewg.org/)
If you are over age 12 and eligible for vaccination, consider protecting yourself and your neighbor with vaccination.
THIS WEBSITE PROVIDES INFORMATION FOR EDUCATIONAL PURPOSES ONLY. CONSULT YOUR HEALTH CARE PROVIDER FOR MEDICAL ADVICE.
Eat clean, drink filtered water, love, laugh, exercise outdoors in a greenspace, get some morning sunlight, block the blue light before bed, engage in meaningful work, find a sense of purpose, spend time with those you love, AND sleep well tonight.
Today’s update from the Johns Hopkins Center for Health Security:
An editorial published in Nature discusses the need to shift focus away from surface decontamination as a mechanism to reduce SARS-CoV-2 transmission risk. Multiple studies have found that transmission of SARS-CoV-2 via contaminated surfaces, or fomites, is relatively rare compared to respiratory transmission via droplets or aerosols. Despite the evidence supporting respiratory exposure as the overwhelming driver of community transmission, numerous public health entities, including the WHO and US CDC, continue to emphasize the importance of surface decontamination, which can cause confusion among the public regarding transmission risk and appropriate protective measures. Notably, surface decontamination efforts, while highly visible and easy to recognize, are costly and likely not effective means of reducing transmission risk. The editorial calls for increased focus on improving ventilation and air filtration capacity to reduce respiratory exposure. Additionally, proper physical distancing and face mask use remain key tools in mitigating exposure and transmission risk for individuals.
The key to reducing the risk of symptomatic infection, especially moderate to severe illness and death appears to be vaccination.
While vaccination clearly reduces the risk of severe illness and death, we do not yet know whether or how much vaccination reduces the risk of carrying and transmitting the virus. So even after vaccination, an asymptomatic or minimally symptomatic person can still transmit the disease to others.
50-60% of viral transmission appears to be from asymptomatic individuals. So wearing a mask, social distancing, and avoiding unventilated crowded indoor spaces remains extremely important.
DOUBLE MASKING IS MORE EFFECTIVE THAN SINGLE MASKS.
A TRIPLE LAYER MASK OF TIGHTLY WOVEN FABRIC IS MORE EFFECTIVE THAN a SINGLE OR DOUBLE LAYER MASK.
N95 MASKS ARE MOST EFFECTIVE BUT THEY MUST FIT THE FACE WITH A TIGHT, SNUG FIT.
TO IMRPOVE THE BARRIER FUNCTION OF MASKS WEAR A SNUG FABRIC MASK OVER A SURGICAL MASK OR OVER AN N-95. THIS WILL PROTECT BOTH THE WEARER AND THOSE AROUND THE WEARER. The fabric mask over a surgical or N-95 mask provides two mechanisms of protection. It adds an extra layer and it provides for a tighter fit of the underlying mask.
Doctors and nurses in hospitals and clinics often wear a surgical mask over an N-95.
Face shields do not protect you or those around you from infection. Face shields and goggles (more so) likely decrease the risk of infection transmitted from aerosols that hit your eyes but do nothing for the most important mechanism of spread, breathing aerosols or droplets into your nose. Aerosols spread around a face shield into your nose.
Think about smelling the pleasant odors of food cooking in a kitchen. Face shields will not block those aerosolized food vapors from entering your nose, but tightly fitting masks will do it to some degree.
SARS-CoV-2 virus is at least 10 times more lethal than an “average” case of influenza. Newer circulating variants have mutations that have probably increased the mortality rate.
SARS-CoV-2 is at least 10 times more easily transmitted compared to most respiratory viruses. Newer circulating variants have definitely increased ease of transmission by at least 30%. As a result, herd immunity will likely require 85-90% vaccination of a given population.
10 times 10 equals 100 TIMES MORE SERIOUS.
In addition, compared to other respiratory viruses, this virus will more frequently cause long lasting or even permanent damage and disability involving one or more organs (heart, lung, kidney, brain). Long-COVID can occur following minimally symptomatic illness and even after asymptomatic illness.
This virus is unique in that TRANSMISSION OCCURS MOST FREQUENTLY FROM ASSYMPTOMATIC INDIVIDUALS.
This occurs for two reasons.
1. Unlike most other respiratory viruses, there is a long time from the onset of when a person becomes infectious to when they become symptomatic. (an average of 5 days)
2. Some individuals never develop symptoms but are still highly infectious for up to 2 weeks.
Restaurants, bars, churches, meeting rooms, cafeterias, parties in closed spaces are situations for SUPERSPREADER EVENTS. An this includes SUPER BOWL PARTIES.
Studies in hospitals show that transmission to health care workers occurs most frequently in the cafeteria and in meeting rooms, not at the bedside where providers are wearing PPE.
In the context of the COVID 19 pandemic I will close with the usual summary.
Exercise, especially out of doors in a green space, supports the immune system
Get some sunshine and make sure you have adequate Vitamin D levels. Supplement with Vitamin D3 to get your levels above 30 ng/ml. (read this Open Letter)
Eliminate sugar-added foods and beverages from your diet. These increase inflammation, cause metabolic dysfunction, and suppress immunity.
Eliminate refined-inflammatory “vegetable oils” from your diet, instead eat healthy fat.
Clean up your home environment and minimize your family’s exposure to environmental toxins by following recommendations at EWG.org with regards to household products, personal care products, and organic foods. (https://www.ewg.org/)
THIS WEBSITE PROVIDES INFORMATION FOR EDUCATIONAL PURPOSES ONLY. CONSULT YOUR HEALTH CARE PROVIDER FOR MEDICAL ADVICE.
Eat clean, drink filtered water, love, laugh, exercise outdoors in a greenspace, get some morning sunlight, block the blue light before bed, engage in meaningful work, find a sense of purpose, spend time with those you love, AND sleep well tonight.
This might explain why lung damage and other organ damage sometimes continues to worsen AFTER the body seems to have cleared the SARS-CoV-2 virus. And it could explain why some individuals fail to mount an adequate immune response early in the disease.
With respect to the later, in September 2020 researchers at the Rockefeller University reported that > 10% of 987 patients with severe COVID-19 infection had antibodies that blocked type 1 interferon molecules, an essential part of the innate immune system.
Other researchers have screened patients with varying severity of COVID-19 and found higher prevalence of autoantibodies against the immune system in infected individuals compared to uninfected controls.
Yet another study found that some infected individuals had autoantibodies against proteins in their blood vessels, heart and brain.
Many patients with severe COVID suffer from life threatening blood clots. Phospholipids play a major role in controlling blood clotting. 52% of 172 people hospitalzied with COVID 19 were found to have anti-phospholipid antibodies.
Annexin A2 is a human protein that protects the integrity of small blood vessels in the lung. Researchers have found a significantly higher average level of anti-annexin A2 antibodies in people who died of COVID-19 compared to patients with less severe illness.
So far it is unclear whether the virus caused these antibodies or whether these unlucky individuals had higher than normal amounts of auto-antibodies prior to infection.
A paper published in the immunology literature just yesterday might shed some light on this issue as well as on the topic of LONG COVID.
We sought to determine whether immune reactivity occurs between anti-SARS-CoV-2 protein antibodies and human tissue antigens, and whether molecular mimicry between COVID-19 viral proteins and human tissues could be the cause.
In other words, they tested antibodies against the SARS-CoV-2 virus to see whether they reacted against various kinds of human tissue. Here is what they found.
We found that SARS-CoV-2 antibodies had reactions with 28 out of 55 tissue antigens, representing a diversity of tissue groups that included barrier proteins, gastrointestinal, thyroid and neural tissues, and more.
This extensive immune cross-reactivity between SARS-CoV-2 antibodies and different antigen groups may play a role in the multi-system disease process of COVID-19, influence the severity of the disease, precipitate the onset of autoimmunity in susceptible subgroups, and potentially exacerbate autoimmunity in subjects that have pre-existing autoimmune diseases.
Cross reactivity between antibodies against COVID-19 virus and human tissue was found for every major organ system in the human body.
The concept of “molecular mimicry” has been well described in auto-immunity for many years. This occurs when a portion of a foreign protein (on for example a virus or bacterium) is identical to a portion of a protein found in human tissue. When the immune system responds to invasion by a virus or bacteria it creates antibodies to various proteins on the invader. But in so doing the anti-bodies can react against human tissue that shares a small common string of amino acids (referred to as an epitope).
A famous example of molecular mimicry occurs with Rheumatic Heart Disease in which antibodies against the bacteria responsible for Strep Throat cross react with heart tissue causing destruction of heart valve tissue and a resultant leaky heart valve. In this situation cross reaction can also occur with tissue in joints resulting in arthritis, another hallmark of rheumatic fever. These were serious complications of Strep Throat before Penicillin became widely available.
So far we know that sicker COVID-19 patients demonstrate antibodies against multiple types of human tissue.
We also know that antibodies that react against various portions of the virus can also react against human tissue.
Finally we know that multi-organ failure is an inflammatory response wherein the immune system, rather than the virus, causes organ failure.
It would be a reasonable conclusion that auto-immunity can acutely contribute to cytokine and bradykinin storm.
It would also be a reasonable conclusion that auto-immunity contributes to LONG COVID.
So why would that make an mRNA vaccine safer?
The mRNA vaccine results in antibodies against one part of the virus (one epitope, the spike protein).
But infection results in antibodies against MULTIPLE PARTS OF THE VIRUS (multiple epitopes). Because multiple antigens or epitopes are involved in the immune response to infection, it increases the probability that cross reaction with multiple human tissues can result.
From an autoimmune perspective, the mRNA vaccine is much safer.
Obviously, given the fact that over 400,000 deaths have resulted in the US from this infection and no deaths have been attributed to the vaccine, the vaccine appears to be much safer than infection. Both the Pfizer and Moderna vaccine have decreased the risk of symptomatic infection by 95%. Severe symptomatic infection can lead to death. Even asymptomatic infection can cause LONG COVID. The risk-benefit analysis overwhelmingly favors the vaccine.
For a deeper dive into auto-immunity and COVID-19 here are a few more references:
Exercise, especially out of doors in a green space, supports the immune system
Get some sunshine and make sure you have adequate Vitamin D levels. Supplement with Vitamin D3 to get your levels above 30 ng/ml. (read this Open Letter)
Eliminate sugar-added foods and beverages from your diet. These increase inflammation, cause metabolic dysfunction, and suppress immunity.
Eliminate refined-inflammatory “vegetable oils” from your diet, instead eat healthy fat.
Clean up your home environment and minimize your family’s exposure to environmental toxins by following recommendations at EWG.org with regards to household products, personal care products, and organic foods. (https://www.ewg.org/)
THIS WEBSITE PROVIDES INFORMATION FOR EDUCATIONAL PURPOSES ONLY. CONSULT YOUR HEALTH CARE PROVIDER FOR MEDICAL ADVICE.
Eat clean, drink filtered water, love, laugh, exercise outdoors in a greenspace, get some morning sunlight, block the blue light before bed, engage in meaningful work, find a sense of purpose, spend time with those you love, AND sleep well tonight.
The new SARS-CoV-2 variant first appearing in southern England has a transmission advantage of 0.4 to 0.7 points higher in reproduction number, also known as R0, compared to the initial strain, British researchers found.
From the study itself:
There is a consensus among all analyses that the VOC has a substantial transmission advantage, with the estimated difference in reproduction numbers between VOC and non-VOC ranging between 0.4 and 0.7, and the ratio of reproduction numbers varying between 1.4 and 1.8.
The researchers published their findings on the school’s website. VOC means “variant of concern”.
In other words, this new variant has an Ro which is 1.4 to 1.8 times higher than the previously circulating predominant strain.
So what is the reproduction number? Ro is the average number of individuals infected by one person. A Ro of 2 means that every infected person on average infects 2 other people.
When a critical proportion of a population becomes immune, called the herd immunity threshold (HIT), the disease no longer spreads exponentially in the population. The disease reaches an endemic steady state. It neither grows nor declines exponentially.
From Wikipedia:
This threshold can be calculated from the effective reproduction number Re, which is obtained by taking the product of the basic reproduction numberR0, the average number of new infections caused by each case in an entirely susceptible population that is homogeneous, or well-mixed, meaning each individual can come into contact with every other susceptible individual in the population,[and S, the proportion of the population who are susceptible to infection, and setting this product to be equal to 1:
Ro X S = 1
S can be rewritten as (1 − p), where p is the proportion of the population that is immune so that p + S equals one. Then, the equation can be rearranged to place p by itself as follows:
Ro x (1-p) = 1, 1-p = 1/Ro, so
When the effective reproduction number Re of a contagious disease is reduced to and sustained below 1 new individual per infection, the number of cases occurring in the population gradually decreases until the disease has been eliminated.
An assumption in these calculations is that populations are homogeneous, or well-mixed, meaning that every individual comes into contact with every other individual, when in reality populations are better described as social networks as individuals tend to cluster together, remaining in relatively close contact with a limited number of other individuals. In these networks, transmission only occurs between those who are geographically or physically close to one another. The shape and size of a network is likely to alter a disease’s HIT, making incidence either more or less common
But transmission is not just affected by the characteristics of the virus, it is also affected by the behavior of the population in which the virus is observed. So it is complicated. As stated by the authors of the transmission study.
We note that these estimates of transmission advantage apply to a period where high levels of social distancing were in place in England; extrapolation to other transmission contexts therefore requires caution.
So if social distancing is relaxed, fewer people wear masks, more people congregate, then this variant could have a much higher Ro.
Ro for measles is 12-18 rendering HIT at 92-95%
Ro for SARS CoV-1 (2002-2004 pandemic) was estimated at 2-5 rendering HIT 50-80%
Ro for SARS CoV-2 (COVID-19) has been estimated at 2.5-4 giving and HIT of 60-75%.
This is not the first variant to demonstrate increased transmission. A new variant emerged in February of 2020 called D614G which had a higher Ro compared to the previously circulating predominant strain. Such strains with higher transmission rates eventually become the predominant strain circulating in a population.
So just as more people suffer from pandemic fatigue and drop their guard we have a more easily transmitted virus. Now is not the time to loosen up on precautions.
In the context of the COVID 19 pandemic I will close with the usual summary.
Eliminate sugar-added foods and beverages from your diet. These increase inflammation, cause metabolic dysfunction, and suppress immunity.
Eliminate refined-inflammatory “vegetable oils” from your diet, instead eat healthy fat.
Clean up your home environment and minimize your family’s exposure to environmental toxins by following recommendations at EWG.org with regards to household products, personal care products, and organic foods. (https://www.ewg.org/)
THIS WEBSITE PROVIDES INFORMATION FOR EDUCATIONAL PURPOSES ONLY. CONSULT YOUR HEALTH CARE PROVIDER FOR MEDICAL ADVICE.
Eat clean, drink filtered water, love, laugh, exercise outdoors in a greenspace, get some morning sunlight, block the blue light before bed, engage in meaningful work, find a sense of purpose, spend time with those you love, AND sleep well tonight.
We must all be thankful for the immunologists who continue to stay on top of the pandemic. They have our backs.
Recent tweets posted by reliable experts who have evaluated the mutations in the B.1.1.7 strain.
We used our database of 579 COVID patient samples to evaluate immune evasion the UK variant (B.1.1.7). Overall takeaway is reassuring: we see no evidence that the reported mutations would substantially increase reinfection risk or decrease vaccine efficacy. (1/n)
Here is some data from the lab of Winn Haynes. @hayneswa
I would prefer this in a manuscript, but given the time of year and that I’m tired, I’ll just tweet the data regarding the UK #COVID19 variant: PRNT50 values from COVID patients for SARS2 WT WA1 vs a mutant that contains N501Y (among other spike mutations).
What does this mean?
In the words of Prof Akiko Iwasaki
As RT above, @TheMenacheryLab has shown functionally that the N501Y mutation in the RBD does not evade existing antibodies’ ability to block replication. (8/n)
Eric Topol:
The good news is that it is not anticipated the current vaccines, which rely on inducing neutralizing antibodies to the spike protein, will be affected by B.1.1.7 or N501Y
If you want to keep up on these issues I suggest you follow Akiko Iwasaki on twitter.
If you want to visit and celebrate, DO IT OUTDOORS with masks and distancing.
Humans need social interaction, this can be done safely without ignoring hygiene recommendations. Socialize and exercise safely outside.
Super-spreader events (such as Whitehouse holiday parties) should be avoided.
Religious services should be held outdoors with precautions. Tents with distancing and masks work!
If you are sick isolate.
Remember, individuals are most infectiousbefore symptoms develop and for the first 5 days after symptom onset. So even though you feel well, you could be a spreader.
Everyone is vulnerable.
Young previously healthy teens and adults are dying and suffering Long-Covid with significant chronic illness.
If you are obese, overweight, pre-diabetic, or have diabetes, now would be a good time to go low-carb with an anti-inflammatory diet. The benefits occur immediately even before or without weight loss.
In the context of the COVID 19 pandemic I will close with the usual summary.
Eliminate sugar-added foods and beverages from your diet. These increase inflammation, cause metabolic dysfunction, and suppress immunity.
Eliminate refined-inflammatory “vegetable oils” from your diet, instead eat healthy fat.
Clean up your home environment and minimize your family’s exposure to environmental toxins by following recommendations at EWG.org with regards to household products, personal care products, and organic foods. (https://www.ewg.org/)
THIS WEBSITE PROVIDES INFORMATION FOR EDUCATIONAL PURPOSES ONLY. CONSULT YOUR HEALTH CARE PROVIDER FOR MEDICAL ADVICE.
Eat clean, drink filtered water, love, laugh, exercise outdoors in a greenspace, get some morning sunlight, block the blue light before bed, engage in meaningful work, find a sense of purpose, spend time with those you love, AND sleep well tonight.
Many would say Albert Einstein, some might suggest Stephen Hawking. But arguably, the greatest might have been a little known, modest but ill-tempered and often vulgar-mouthed virologist named Maurice Hilleman.
Hilleman’s twin sister died at birth, his mother died 2 days later. His father gave him over to his aunt and uncle and he worked their farm in Montana. For want of funds he deferred college until his brother returned from divinity school and convinced him to attend Montana State. He was raised in a deeply religious family and was observed to read Darwin’s Origin of the Species while in church as a teenager.
He went on to graduate school for microbiology and discovered that Chlamydia, previously thought to be a virus, was an intra-cellular bacteria.
Shortly after graduate school and at the request of the US military he developed a vaccine for Japanese Encephalitis which was wreaking havoc with US soldiers in the Pacific during WW2.
He made a list of serious childhood illnesses and decided to devote his life to developing vaccines for all of them.
The story of the mumps vaccine is fascinating. His daughter developed mumps. He swabbed her throat, took the sample to his lab and cultured the virus in chicken embryo cells. Over 2 years he developed a series of virus mutations in successive dishes of embryo cells. Each virus culture became less virulent for humans. This had never been done before. Eventually, he had a “live-attenuated” virus that could be used for human vaccination.
His work was performed under what would now be considered primitive scientific conditions but it was state of the art for his time.
It has been estimated that his work saves over 8 million lives every year.
Paul Offit MD, Director of Vaccine Development at Children’s Hospital in Philadelphia (U Penn.) a present day preeminent vaccinologist, spent 72 hours interviewing Maurice Hilleman when he was dying from cancer, to record his amazing history.
The folks who worked for Maurice Hilleman were intensely loyal. He was totally devoted to science and vaccine development. Yet on the day he died, Paul Offit walked into a room filled with pediatricians where he was giving a lecture and not one pediatrician knew who he was or what he had accomplished.
From Wikipedia:
Robert Gallo, co-discoverer of HIV, the virus that causes AIDS, once said “If I had to name a person who has done more for the benefit of human health, with less recognition than anyone else, it would be Maurice Hilleman. Maurice should be recognized as the most successful vaccinologist in history.”[14]
After Hilleman’s death Ralph Nader wrote, “Yet almost no one knew about him, saw him on television, or read about him in newspapers or magazines. His anonymity, in comparison with Madonna, Michael Jackson, Jose Canseco, or an assortment of grade B actors, tells something about our society’s and media’s concepts of celebrity; much less of the heroic.”[15]
Eliminate sugar-added foods and beverages from your diet. These increase inflammation, cause metabolic dysfunction, and suppress immunity.
Eliminate refined-inflammatory “vegetable oils” from your diet, instead eat healthy fat.
Clean up your home environment and minimize your family’s exposure to environmental toxins by following recommendations at EWG.org with regards to household products, personal care products, and organic foods. (https://www.ewg.org/)
THIS WEBSITE PROVIDES INFORMATION FOR EDUCATIONAL PURPOSES ONLY. CONSULT YOUR HEALTH CARE PROVIDER FOR MEDICAL ADVICE.
Eat clean, drink filtered water, love, laugh, exercise outdoors in a greenspace, get some morning sunlight, block the blue light before bed, engage in meaningful work, find a sense of purpose, spend time with those you love, AND sleep well tonight.
This week began the saga of vaccine implementation for the mRNA vaccine developed by the Pfizer-BioNtech partnership. The New England Journal of Medicine published a peer-reviewed article reporting the data from the RCT (Randomized Controlled Trial) and an Editorial appeared on the same day in the NEJM. You can view both here:
Here is the most important table in the peer-reviewed article:
Age > 55 includes >=65 and >=75, Age >= 65 includes age >=75. If age>= 75 were not listed separately, all age groups would have statistical significance. This is why overall number of infections in the vaccine group is 8 but the total of the four age groups is 9. One of the 3 infections in age >55 was 65 or older. Got it?
Look at the third column labeled “Surveillance Time”. The first number in this column is described under the caption as “total time in 1000 person-years for the given endpoint..” So multiply by 1000 and you get a number that represents “person years” of observation. This is an odd number but a reasonable way to present information. The trial data covers a period of 6 months starting from when the first patient was vaccinated. The median duration of observation was 2 months after vaccination with the second dose. (50% of patients had been vaccinated for more than 2 months and 50% of patients less than 2 months)
The number in parentheses gives the number of people in each category of age, sex, race/ethnic group, country.
Notice that as we descend through the age groups from youngest to oldest, the number of participants decreases significantly in >= 65 and >=75 years old.
Now go to the last column labeled “Vaccine Efficacy, %”. The first number is the overall efficacy for that age group. But how confident are we about that efficacy % for each age group? The numbers in the parentheses represents a range or “confidence interval” which is determined statistically. This range is determined by the number of people in each (age) group and by the difference between the placebo and drug treatment outcome in that age group.
Note that the confidence interval widens as you go down from younger to older age groups. That is primarily because the number of people represented by the groups age >=65 and >= 75 are much smaller than the first two age groups.
For the age group > 65, the efficacy is reported at 94.7%. But that is an average number that shows that compared to the placebo group, the symptomatic infection rate in the vaccinated group was 94.7% lower. For the age group between >=65, there were 19 cases of symptomatic infection in the placebo group and only 1 in the vaccine group. 1/19 equals 0.0526. 1 minus 0.0526 equals 0.947 or 94.7% (rounding).
What is a 95% confidence interval?
The 95% confidence interval is the the range over which we are 95% confident the “true” value falls within. In other words, for age >=65 there is a 95% probability that the true vaccine efficacy falls somewhere between 66.7% and 99.9%. As more people age >=65 are entered into the trial, the confidence interval will get narrower for that age group provided the difference between the placebo and vaccine group remains the same. If the difference between placebo and vaccine groups increases AND the number of people in this age group increases, the confidence interval will shrink further.
This is a fantastic result!
But now look at the confidence interval for age >=75. It is -13.1-100. A minus number is in the range. That means we do not have enough people in the study age 75 or older to reach a “statistically significant” conclusion. There were only 774 folks who received the vaccine and 785 people who received the placebo in this age group. 5 in the placebo group got sick, 1 in the vaccine group got sick. This difference shows a “trend” but does not reach “statistical significance”. We need more data for this group.
But again, do not lose heart. Based on this data, which includes efficacy and safety overall, I recommend that my 92 year old mother-in-law receive the vaccine as soon as it is available.
What is “statistical significance”?
Simply stated, a result is “statistically significant” in a drug trial if the probability that the difference between the placebo group and the drug group occurred by accident (or by chance) is less than or equal to 5%. Or to put it another way, the probability that the difference between placebo and drug did not occur by chance but rather represents a true difference in outcome is 95% or greater. 5% is the standard cutoff point in medical trials. This is usually reported as a “p value”. If a p value is less than or equal to 0.05 the difference is considered statistically significant.
“Clinical significance” is another issue. For example, a drug might only decrease relative risk of an event by 5%, but the result could be “statistically significant”.
In the case of this vaccine, the clinical significance is outstanding.
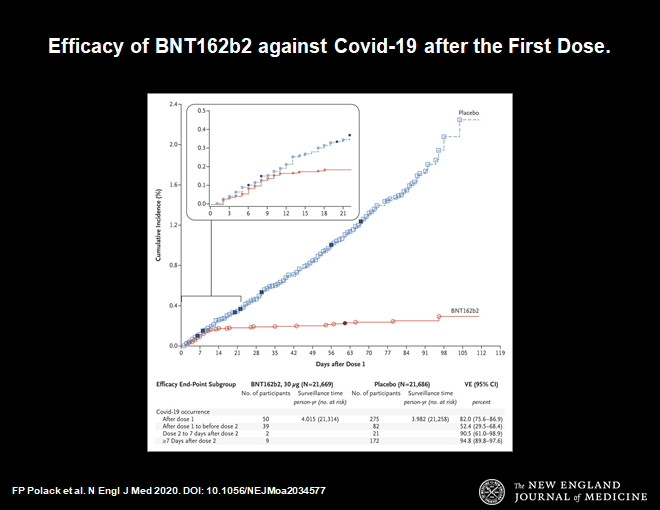
Here is another important chart.
Protection begins at day 14 after first dose
This chart demonstrates that 14 days after the first dose of vaccine protection from symptomatic infection begins. The blue line shows infections in the placebo group, the red line is the vaccine group. They diverge at day 14. Thereafter the divergence increases. This makes sense. It is consistent with our understanding of how the immune system works. This time course is very reassuring.
Now let us look at side effects.
These are the usual side effects expected with any vaccine. Symptoms such as fever, malaise, local reaction at the injection site, muscle aches are all to be expected. This profile is a little worse than the flu vaccine, but less compared to the shingles vaccine.
So far 2 episodes of anaphylaxis have occurred in the US and in UK with the vaccine rollout. (millions of doses already given) This can happen with any vaccine, that is why 15 minutes of observation following vaccination is part of the protocol and the vaccine should only be administered in a location that has epinephrine available to treat a severe allergic reaction.
This vaccine time sequence is historically unprecedented. This was made possible by a combination of advances in science and incredible action on the part of the public and private sectors in response to a global crisis. Prior to this, the shortest time to develop an effective vaccine was 4.5 years (measles mumps, and that was done by Maurice Hilleman with the help of a few lab assistants, more about Maurice in my next post).
I received my first dose of the vaccine today (as a member of hospital medical staff). I was directed to a CDC website to register as a vaccine recipient. The CDC will send me periodic questions on side effects which I will answer. If everyone participates in this program more data will become available on safety and efficacy. So please participate when you get the vaccine (vsafe.cdc.gov).
Many questions remain. Here is a quote from the NEJM editorial:
Will unexpected safety issues arise when the number grows to millions and possibly billions of people?
Will side effects emerge with longer follow-up?
Implementing a vaccine that requires two doses is challenging. What happens to the inevitable large number of recipients who miss their second dose?
How long will the vaccine remain effective?
Does the vaccine prevent asymptomatic disease and limit transmission?
And what about the groups of people who were not represented in this trial,such as children, pregnant women, and immunocompromised patients of various sorts?
The logistic challenges of manufacturing and delivering a vaccine remain daunting. This vaccine, in particular, requires storage at −70°C, a factor that may limit its deployment in some areas. Nevertheless, the remarkable level of safety and efficacy the vaccine has demonstrated thus far make this a problem that we should welcome solving. What appears to be a dramatic success for vaccination holds the promise of saving uncounted lives and giving us a pathway out of what has been a global disaster.
In the context of the COVID 19 pandemic I will close with the usual summary.
Eliminate sugar-added foods and beverages from your diet. These increase inflammation, cause metabolic dysfunction, and suppress immunity.
Eliminate refined-inflammatory “vegetable oils” from your diet, instead eat healthy fat.
Clean up your home environment and minimize your family’s exposure to environmental toxins by following recommendations at EWG.org with regards to household products, personal care products, and organic foods. (https://www.ewg.org/)
THIS WEBSITE PROVIDES INFORMATION FOR EDUCATIONAL PURPOSES ONLY. CONSULT YOUR HEALTH CARE PROVIDER FOR MEDICAL ADVICE.
Eat clean, drink filtered water, love, laugh, exercise outdoors in a greenspace, get some morning sunlight, block the blue light before bed, engage in meaningful work, find a sense of purpose, spend time with those you love, AND sleep well tonight.