Trump has recently accused doctors of falsifying death certificates for financial gain. Let’s be clear.
If a patient is hospitalized with viral pneumonia and dies, the cause of death has ALWAYS been listed as the viral pneumonia, no matter what complications occurred, no matter what the pre-existing conditions were. Viral pneumonia can cause heart attack, stroke, kidney failure, multiple organ failure but the proper cause of death to be listed is the initial presenting causative agent.
Doctor’s caring for COVID-19 patients in the hospital do not get paid more because of the diagnosis. Hospitals may get extra payment because of the pandemic circumstances, doctors do not. Recently the AMA has recommended additional payment to OFFICE PRACTICES for the extra expense of COVID-19 precautions. This does not impact hospital doctor payment.
Death is not the only bad outcome. “Long COVID” is a state of persistent symptoms and disability that can occur even after mild illness not requiring hospitalization. Post viral syndromes such as this have long been recognized and can last a lifetime. Consequences can include shortness of breath with minimal exertion, chronic fatigue, heart failure, kidney failure, chronic pain to name a few. A recent study from Germany demonstrated MYOCARDITIS (chronic heart inflammation) in 70% of patients “recovered” from COVID-19. 80% of those patients were not hospitalized. We do not yet know the extent of long term morbidity caused by this virus. Viral Myocarditis is a common cause of cardiomyopathy that can lead to heart transplant, shortened life, and decreased quality of life.
Misleading and untruthful statements that downplay the serious nature of this pandemic, especially by national leadership, cause great harm to our nation, bringing unnecessary death, suffering, and economic ruin. Such lies result in many people defying necessary and effective public health measures such as wearing masks, washing hands, social distancing.
In any pandemic public health recommendations change as more information becomes available. This is to be expected. Trump has dangerously and tragically criticized our public health leaders for changing recommendations as new information and new circumstances have evolved.
The greatest nation in the world still has not implemented an adequate TEST-TRACE-ISOLATE infrastructure. Our testing is inadequate, takes too long, has too many false positives and false negatives. Similarly, tracing and isolating are not widely and effectively implemented. This requires NATIONAL COORDINATION AND LEADERSHIP. It also requires that all Americans take this seriously. Trumps denial of the truth has led many Americans to disregard the necessary steps to safely reopen our economy.
By now business shut downs and severe restrictions would be unnecessary if America had instituted early and effective TEST-TRACE-ISOLATE. By now, our economy would be out of trouble. Instead lies, deceit, and incompetence has led to unnecessary death, suffering, chronic illness, and economic disaster.
Even after a vaccine is available, MASKS, HAND WASHING, SOCIAL DISTANCE, will still be necessary for a long time.
The Republican leadership has consistently failed to call out TRUMP on this issue and many others. The Republican leaders have failed to fulfill their sworn duty to protect our citizens from harm and instead placed party over country. This deplorable behavior threatens Balance of Power and Democracy itself.
In the context of the COVID 19 pandemic I will close with the usual summary.
Eliminate sugar-added foods and beverages from your diet. These increase inflammation, cause metabolic dysfunction, and suppress immunity.
Eliminate refined-inflammatory “vegetable oils” from your diet, instead eat healthy fat.
Clean up your home environment and minimize your family’s exposure to environmental toxins by following recommendations at EWG.org with regards to household products, personal care products, and organic foods. (https://www.ewg.org/)
THIS WEBSITE PROVIDES INFORMATION FOR EDUCATIONAL PURPOSES ONLY. CONSULT YOUR HEALTH CARE PROVIDER FOR MEDICAL ADVICE.
Eat clean, drink filtered water, love, laugh, exercise outdoors in a greenspace, get some morning sunlight, block the blue light before bed, engage in meaningful work, find a sense of purpose, spend time with those you love, AND sleep well tonight.
If we continue to grow crops and raise animals the way we presently do, our topsoil will be gone in 20 years! There will be another dustbowl but this time it will be NATIONWIDE.
Shocking? Yes.
Fake news? NO.
Watch this 2.5 minute trailer to understand the scope of this problem and the simple proven solution that will not only lead to carbon sequestration in the ground but will create soil and improve the profitability of farming and ranching.
Watch this movie to understand why we must create soil with regenerative farming and ranching.
When we destroy soil and turn it into dirt we release CO2 into the atmostphere.
When we create living soil, returning insects, microbes, viruses, worms, fungi and water to their proper ecosystem role, we capture CO2 from the atmosphere and sequester it in the newly created soil through the crops. Moving CO2 from air to plant to soil through the roots, that is the path to saving out planet and providing for world-wide food security.
Biosequestration is the process of using plants, trees, and techniques of farming and raising animals, to capture carbon and store it in the soil. Restoration of grasslands along with regenerative agriculture can accomplish this much quicker and with greater return on investment than planting trees. Of course restoring forests should also be part of a global effort to save our planet from destruction. But the quickest, most efficient way to solve multiple problems at once is to convert present day mono-agriculture system that destroys soil releasing CO2 into the air with the opposite and more profitable system of regenerative agriculture and ranching.
But what about eating meat and raising cattle? We have heard that is bad for the planet. THE SCIENCE SAYS OTHERWISE.
You can watch this BRIEF TRAILER:
That is the science.
Plants capture CO2 and put it back into the soil. Plants and soil capture and sequester rain water as well as CO2, further preventing erosion and runoff. But to create soil we need ruminant animal poop!!!!!!!!!!!
Regenerative agriculture and ranching avoids fossil-fuel based fertilizer and toxic chemicals and uses instead manure from grazing animals to fertilize crops and convert dirt into living soil. This process creates life and habitat for numerous species of animals, plants, microbes etc.
This is a win-win scenario.
What stands in the way?
Ignorance, habit, and Federal subsidy of corn, wheat, soy.
Most (>90%) of the (subsidized) grains grown in the US go into feeding cattle and pigs which are raised on factory farms. After grazing naturally during their early life, most cattle are then moved onto feedlots to be fed GMO glyphosate-resistant grains which degrade the quality of their fat and protein and transfer toxic glyphosate from grain to animal. Those cattle stand in their own excrement and require antibiotics to fend off the inevitable infections that come with feedlot conditions.
The pigs live their lives in a warehouse standing on grated floors dropping their excrement into methane producing lakes of pig poop which overflow into streams and rivers when heavy rains fall.
Antibiotic resistant organisms are created in our feed lots and contribute to our epidemic of antibiotic resistant infections in humans.
But it need not be that way.
After viewing the trailers linked above, watch the movies KISS THE GROUND (already released and available on Netflix) and Sacred Cow (soon to be released) you will learn the path to recovering the health of our planet and the health of our human population.
If you still do not believe this narrative or want to dive deeply into the science, read the book:
“Data from farming and grazing studies show the power of exemplary regenerative systems that, if achieved globally, would drawdown more than 100% of current annual CO2 emissions.”
That is a very bold but hopeful statement, backed by solid science. It will improve the bottom line for farmers and ranchers by increasing production per acre with non-toxic, soil producing simple farmer’s almanac based technology already being practiced and proven today.
“Actual yields in well-designed regenerative organic systems, rather than agglomerated averages, have been shown to outcompete conventional yields for almost all food crops including corn, wheat, rice, soybean, and sunflower.”
Finally, the scoop on methane produced by cattle and the difference between that and fossil fuel generated CO2 is discussed in this very brief animation.
Eliminate sugar-added foods and beverages from your diet. These increase inflammation, cause metabolic dysfunction, and suppress immunity.
Eliminate refined-inflammatory “vegetable oils” from your diet, instead eat healthy fat.
Clean up your home environment and minimize your family’s exposure to environmental toxins by following recommendations at EWG.org with regards to household products, personal care products, and organic foods. (https://www.ewg.org/)
THIS WEBSITE PROVIDES INFORMATION FOR EDUCATIONAL PURPOSES ONLY. CONSULT YOUR HEALTH CARE PROVIDER FOR MEDICAL ADVICE.
Eat clean, drink filtered water, love, laugh, exercise outdoors in a greenspace, get some morning sunlight, block the blue light before bed, engage in meaningful work, find a sense of purpose, spend time with those you love, AND sleep well tonight.
In a previous post I praised the recently released book SACRED COW which discusses regenerative agriculture, creation rather than destruction of soil through better farming models, the need for cattle (ruminants) in soil creation, the myths concerning vegetarian diets-saving-the-planet, and many issues related to nutrition and health of the planet.
A recently published white paper on the topic of regenerative agriculture states “there is hope right beneath our feet” to address the climate crisis and global food security at the same time.
The most profound conclusion of this paper provides hope for the climate crisis:
“Data from farming and grazing studies show the power of exemplary regenerative systems that, if achieved globally, would drawdown more than 100% of current annual CO2 emissions.”
Regenerative agriculture is
“a system of farming principles that rehabilitates the entire ecosystem and enhances natural resources, rather than depleting them.”
Comparing regenerative agriculture to present day industrial farming an eco-artist has created this image.
Mono-agriculture on the left, Regenerative agriculture on the right.
“In contrast to industrial practices dependent upon monocultures, extensive tillage, pesticides, and synthetic fertilizers, a regenerative approach uses, at minimum, seven practices which aim to boost biodiversity both above and underground and make possible carbon sequestration in soil.
Diversifying crop rotations
Planting cover crops, green manures, and perennials
Retaining crop residues
Using natural sources of fertilizer, such as compost
Employing highly managed grazing and/or integrating crops and livestock
Reducing tillage frequency and depth
Eliminating synthetic chemicals”
“When compared to conventional industrial agriculture,” the authors write, “regenerative systems improve”:
Biodiversity abundance and species richness
Soil health, including soil carbon
Pesticide impacts on food and ecosystems
Total farm outputs
Nutrient density of outputs
Resilience to climate shocks
Provision of ecosystem services
Resource use efficiency
Job creation and farmworker welfare
Farm profitability
Rural community revitalization
A movie KISS THE GROUND, highlights the importance of a transition from present day mono-agriculture to a Regenerative approach. You can view the trailer here.
Along these lines, be on the lookout for a similar movie version of the book SACRED COW.
The US military has determined that the greatest threat to global security is CLIMATE CHANGE.
Alternative energy sources and elimination of fossil fuels can cut our carbon emissions but will not sequester the carbon in our atmosphere. REGENERATIVE AGRICULTURE can sequester carbon, create new living soil, and feed the planet a healthy diet.
The following short animation explains the difference between methane from cows and CO2 from burning fossil fuels. The “natural carbon cycle” reveals the difference.
Eliminate sugar-added foods and beverages from your diet. These increase inflammation, cause metabolic dysfunction, and suppress immunity.
Eliminate refined-inflammatory “vegetable oils” from your diet, instead eat healthy fat.
Clean up your home environment and minimize your family’s exposure to environmental toxins by following recommendations at EWG.org with regards to household products, personal care products, and organic foods. (https://www.ewg.org/)
THIS WEBSITE PROVIDES INFORMATION FOR EDUCATIONAL PURPOSES ONLY. CONSULT YOUR HEALTH CARE PROVIDER FOR MEDICAL ADVICE.
Eat clean, drink filtered water, love, laugh, exercise outdoors in a greenspace, get some morning sunlight, block the blue light before bed, engage in meaningful work, find a sense of purpose, spend time with those you love, AND sleep well tonight.
That is where we have failed. Those countries that rapidly instituted masks, social distance, frequent hand washing, PLUS Test/Trace/Isolate succeeded in limiting the speed of spread, protected the Medical Care (hospital) system from being over-run, and protected it’s citizens and economy. Those countries bought time to learn enough about the virus to lower the mortality rates by developing treatments that decrease risk of death AND probably disability and to ramp up the hospital care system and PPE.
The US has failed to meet the challenge.
Death may not be the worst outcome, depending on one’s views relative to the balance between longevity and quality of life. Chronic disability (such as congestive heart failure, severe pulmonary insufficiency, kidney failure requiring dialysis, stroke, etc.) can be lifelong and devastating following this infection. Some may consider that shortness of breath after walking 100 feet, requiring a rest before moving on, or kidney dialysis 3 times per week the price one must pay to survive a serious infection. Others may think this sort of severe disability is not acceptable. Many in our society are clueless about these potential outcomes (usually that means they are in denial, a very common defense mechanism used to deal with a terrible threat).
This did not have to be our present state, but it is.
In December US intelligence agencies (including the CIA) and the US military intelligence were already issuing reports about an emerging deadly respiratory virus in China. This went up the chain of command but was ignored by the Whitehouse. In January, Doctor Fauci, at the annual BIOTHREATS CONFERENCE in Washington DC, announced to the bio-tech industry representatives in attendance that this virus was already “beyond containment” and stated that aggressive biomedical development (drugs, vaccines, etc.) would be required. He told attendees that the NIH would “find the money” to support these efforts and that this was a national and global emergency.
Undoubtedly, this was reported to the Whitehouse. These early warnings were not only ignored, they were also widely denied publicly by our highest public official. (The warnings issued in senatorial and congressional committee meetings however, prompted many privileged senators and congress people to sell pandemic-sensitive stocks very early in the “denial phase”).
It is clear that masks and social distancing are effective in limiting spread. Super-spreader cases, case studies of spread in restaurants (China) , call centers (South Korea), and choir rehearsals (Washington State) suggest that both droplet and aerosol transmission occur in non-medical procedure settings.
We already knew that aerosol spread occurred in operating rooms when nasopharyngeal surgery and similar aerosol generating medical procedures were performed. In one operating room event, all 11 doctors and nurses who spent any amount of time in that operating room (despite everyone wearing N95 masks) became infected and the surgeon died from the infection (he had the most exposure). This was reported early on documenting aerosol spread in medical settings.
For those who have not read my previous discussion of aerosol vs droplet spread:
Aerosol = very small lighter-than-air particles containing infectious virus that float in the air and can be recirculated through air-conditioning vents or linger suspended in the air, especially indoors where the air is still.
Droplets = larger particles that fall quickly onto surfaces but can also with a cough, sneeze, scream or singing be transmitted to someone in very close proximity before falling .
Then we learned that carriers/transmitters of the virus can either remain completely without symptoms or develop symptoms as late as 10 days after initial exposure, all the while transmitting the virus to others around them. Assymptomatic transmission makes COVID 19 different from and more dangerous than most other viruses that infect humans.
Let me say that again.
Aerosol transmission makes this virus more dangerous than most other viruses.
Asymptomatic transmission makes this virus more dangerous than most other viruses.
And finally we have learned that this virus is more lethal than most other viruses. For example, COVID 19 is 25 times more lethal than the H1N1 influenza pandemic (references provided in previous post).
To summarize, the combination of easy transmission, asymptomatic transmission, and high mortality rate make this virus exceptionally dangerous and difficult to control.
How did the US respond?
Instead of rapidly ramping up PPE, testing, tracing, and isolation public health capability we instead had national leadership that said this was just like “another flu” virus and would “go away”. The narrative constantly shifted, but more importantly, effective action was not taken, and still has not been taken.
Testing remains woefully inadequate.
In many areas of our country it can take 5 days to schedule a test and 10 days to get the results. Such tests are useless. To effectively implement TEST/TRACE/ISOLATE we need rapid and widespread testing, rapid reporting, and a system to then trace contacts and isolate infected and exposed individuals. The US still shamefully lacks these essential services.
John’s Hopkins University early on developed an on-line contact tracing training program. But public funding to hire such trained individuals has been inadequate.
Isolation requires facilities in which exposed or infected individuals have their own bathroom and bedroom, have food provided, and are medically supervised until they are no longer infectious.
The US does not have such facilities. Individuals, unless they are financially very secure, do not have access to a home or other environment where this is possible. Worse, those essential workers (meat packers, food delivery, nursing aids, etc.) who earn the least, usually live in cramped housing conditions with multi-generation households in which isolation is impossible. Such individuals often live from paycheck to paycheck, so staying home from work means the family does not eat or the rent is not paid. So they go to work infecting others.
The result has been not just death and disability but horrible economic consequences.
Our shutdowns could have been shorter had we acted quickly and effectively.
Had we responded rapidly and appropriately, we would not be in our present economic predicament. So ironically and tragically, those that complain that shutdowns “were not necessary” and masks “are not necessary” contribute to the worsening economic consequences. As the virus surges following relaxation of restrictions, further restrictions and economic consequences become necessary.
Compounding this situation is the denial on the part of many individuals regarding the science and facts about this virus. Part of this denial is the result of our con-artist in chief, (and some governors) misrepresenting the facts to the public and displaying inappropriate behavior (such as refusal to wear a mask until most recently).
The other component of this denial is based on the natural tendency of humans to ignore data that is threatening and not consistent with personal ideology and beliefs. Beliefs such as “the government lies, the government is not to be trusted, the government cannot tell me what to do” presents obstacles to social behavior that would protect not just oneself and family, but the community (and economy) in general.
Contact tracers have reported that sometimes people hang up on them, refuse to cooperate, sometimes saying that it is an “invasion of privacy” or a “government hoax”.
Such beliefs and behaviors are encouraged by misinformation in the social media, shock-jocks such as Rush Limbaugh, conspiracy theories, and supported by dangerous politicians who have placed party over country, ideology over science, the next election over the good of the country.
The best way to mitigate the dire health and ECONOMIC CONSEQUENCES of this pandemic include all those components that have worked in other countries:
MASKS4ALL
SOCIAL DISTANCE
FREQUENT HAND WASHING
SOCIAL BUBBLE
TEST/TRACE/ISOLATE
This is a sad state. In the meantime what can you do?
In the context of the COVID 19 pandemic I will close with the usual summary.
Eliminate sugar-added foods and beverages from your diet. These increase inflammation, cause metabolic dysfunction, and suppress immunity.
Eliminate refined-inflammatory “vegetable oils” from your diet, instead eat healthy fat.
Clean up your home environment and minimize your family’s exposure to environmental toxins by following recommendations at EWG.org with regards to household products, personal care products, and organic foods. (https://www.ewg.org/)
THIS WEBSITE PROVIDES INFORMATION FOR EDUCATIONAL PURPOSES ONLY. CONSULT YOUR HEALTH CARE PROVIDER FOR MEDICAL ADVICE.
Eat clean, drink filtered water, love, laugh, exercise outdoors in a greenspace, get some morning sunlight, block the blue light before bed, engage in meaningful work, find a sense of purpose, spend time with those you love, AND sleep well tonight.
The USDA Dietary Guidelines are about to be published again with an update. Unfortunately, despite much input from the scientific community requesting that the dietary guidelines address the epidemics of obesity and diabetes, it looks like nothing will change. More than 50 scientific papers that support a Very Low Carbohydrate approach to address obesity, diabetes and pre-diabetes will be ignored.
But if you want a more scientific perspective I suggest you watch this movie. You can watch it free on Amazon Prime.
Both books are well researched and present accurate science. The movie Fat Fiction reviews the sad history of dietary advice in the US. It presents many examples of patients whose lives were changed and improved by following the advice of nutritionists and physicians who have instead, followed the science and abandoned the ideological-unscientific USDA dietary guidelines.
The American Diabetes Association has finally recognized a VLC ketogenic diet as a valid approach to treating type 2 diabetes. In fact, a ketogenic diet is the only diet that has ever been documented in controlled clinical trials to reverse diabetes type 2 and get patients off insulin and oral medications used to treat diabetes.
Unfortunately, the USDA guidelines and the American Heart Association recommendations continue to recommend unhealthy inflammatory refined “vegetable oils” (processed/refined oils from corn, soy, safflower, peanuts, cottonseed, etc.) and high carbohydrate/low fat meals. The high carb/low fat approach to cardiovascular disease, obesity, and diabetes has been an absolute failure, increasing rather than decreasing the risk of heart attack and stroke as well as contributing to the explosive epidemics of obesity and DM2. The low fat dogma has fostered the obesity and diabetes epidemics since this dogma was first introduced in the mid 20th century. The low-fat ideology remains fully supported by financial contributions from the processed-food industry, creating a financial conflict of interest for the AHA and similar organizations.
In the context of the COVID 19 pandemic, where obesity, insulin resistance, pre-diabetes and diabetes type II are major risk factors for death from the infection, it is even more imperative that individuals suffering from these risk factors stop using medications to treat problems created by food and instead clean up their diet.
“You can’t throw drugs at a nutritional disease and expect it to work” (Dr. Sarah Hallberg, TEDtalk)
You can fight systemic inflammation with the anti-inflammatory diet I present on this website, but if you have obesity, diabetes or pre-diabetes, the very low-carb version is the most effective and sustainable nutritional approach. Full fat dairy is optional (although technically not part of our evolutionary nutrition) and if you are obese, overweight, diabetic or pre-diabetic and full fat dairy is necessary for you to achieve a ketogenic diet, then go for it. But make sure you include an abundance of non-starchy vegetables which are an important component of a healthy ketogenic diet.
In the context of our present pandemic I will repeatedly say:
Eliminate sugar-added foods and beverages from your diet. These increase inflammation, cause metabolic dysfunction, and suppress immunity.
Eliminate refined-inflammatory vegetable oils from your diet, instead eat healthy fat.
Clean up your home environment and minimize your family’s exposure to environmental toxins by following recommendations at EWG.org with regards to household products, personal care products, and organic foods. (https://www.ewg.org/)
THIS WEBSITE PROVIDES INFORMATION FOR EDUCATIONAL PURPOSES ONLY. CONSULT YOUR HEALTH CARE PROVIDER FOR MEDICAL ADVICE.
Eat clean, drink filtered water, love, laugh, exercise outdoors in a greenspace, get some morning sunlight, block the blue light before bed, engage in meaningful work, find a sense of purpose, spend time with those you love, AND sleep well tonight.
This discussion was originally posted before PAXLOVID WAS AVAILABLE. Paxlovid is very effective in reducing morbidity and mortality associated with Covid-19 infection. Standard dosing: PAXLOVID two 150-mg tablets of nirmatrelvir, one 100-mg tablet of ritonavir twice daily for 5 days.
Dose adjustments are necessary for certain medical conditions and there are many drug interactions that should be considered.
The results of a randomized placebo controlled clinical trial in high risk individuals has been published in the NEJM. The study was done just when Omicron hit. The study demonstrated an 89% reduction of hospitalizations and deaths by day 28 (absolute reduction of 6.2/100) with ZERO deaths in the Paxlovid group (7 in the placebo group). Paxlovid also had LESS side effects than placebo.
Another study from Israel demonstrated equally impressive results as shown here.
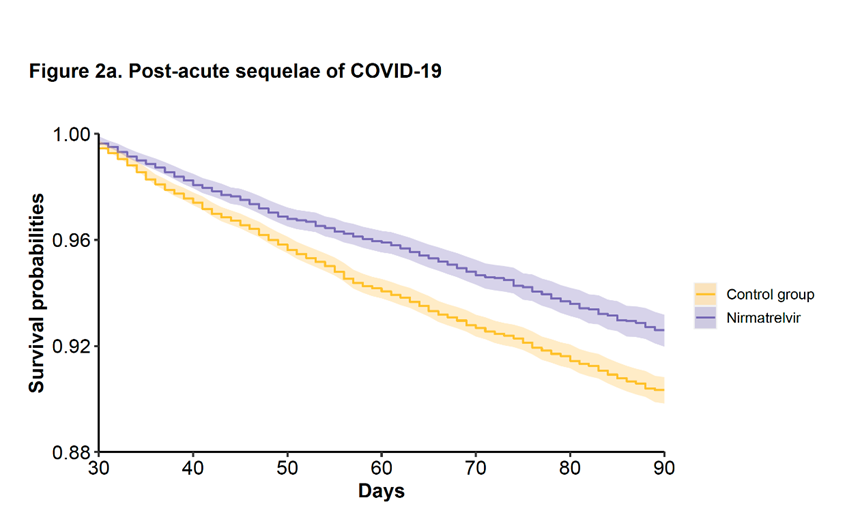
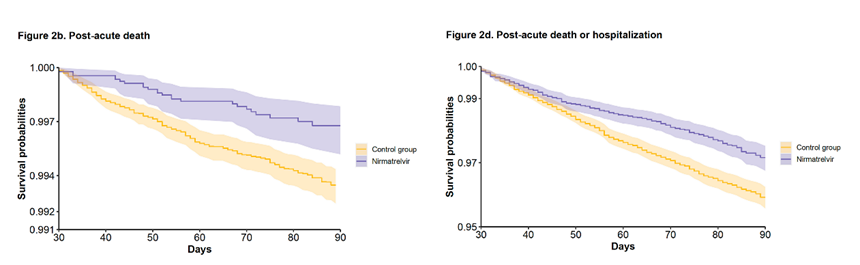
In addition, a study from the VA has looked at longer term effects (pre-print publication, still waiting for peer review.)
The study included 9000 Paxlovid patients treated within 5 days of symptom onset during the Omicron and subvariant waves and compared the treated patients with approximately 47,000 matched controls.
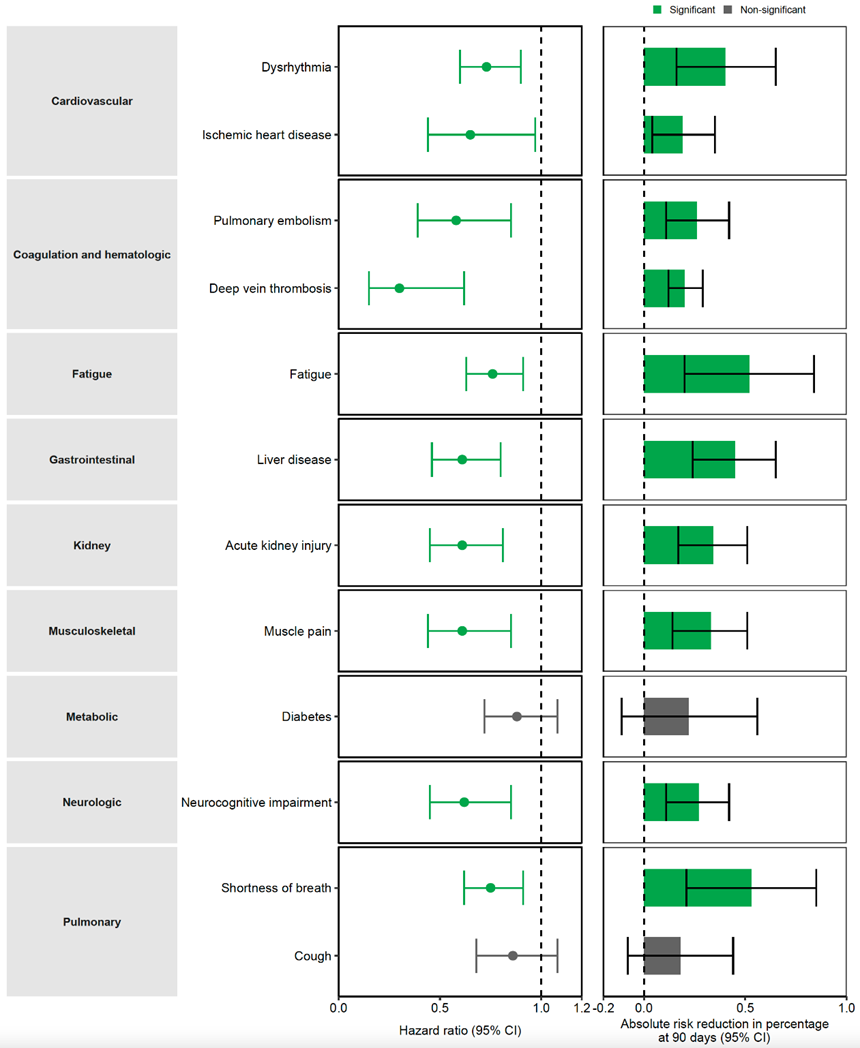
There was a 26% reduction in Long Covid.
Here is a breakdown of the Long Covid Symptoms
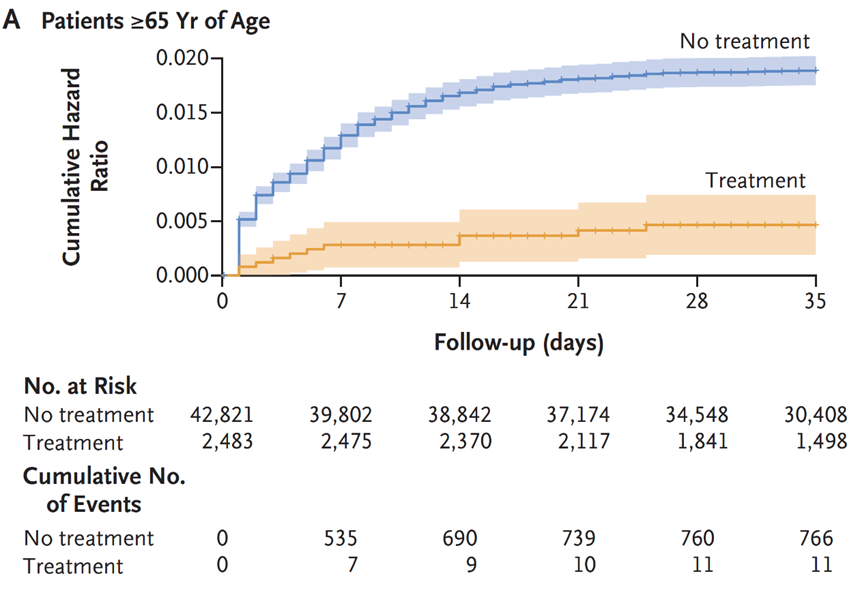
The VA study also showed a 48% reduction of death and 30% reduction in hospitalization after the acute phase (acute phase = first 30 days) as demonstrated here.
Many drug intervention trials for treating COVID-19 early in the pandemic have been disappointing. No studies have shown benefit for hydroxychloroquine, with or without azithromycin. This topic has been covered in previous posts. Remdesivir was FDA approved based upon one study that showed reduction in duration of symptoms. The mortality rate with Remdesivir, however, did not demonstrate a statistically significant difference when compared to “usual care”. https://www.niaid.nih.gov/news-events/nih-clinical-trial-shows-remdesivir-accelerates-recovery-advanced-covid-19
Another study published in Lancet failed to show any clinical benefit from Remdesivir.
“No statistically significant benefits were observed for remdesivir treatment beyond those of standard of care treatment. Our trial did not attain the predetermined sample size because the outbreak of COVID-19 was brought under control in China. Future studies of remdesivir, including earlier treatment in patients with COVID-19 and higher-dose regimens or in combination with other antivirals or SARS-CoV-2 neutralising antibodies in those with severe COVID-19 are needed to better understand its potential effectiveness.”
Likewise well designed studies of Ivermectin have shown no clinical benefit.
Monoclonal antibodies effective against early variants are no longer effective against the newer variants. So in terms of drug therapies for acute Covid infections we have Paxlovid for out patient care and dexamethasone for critically ill patients.
But we do know that certain underlying conditions such as obesity, diabetes, pre-diabetes (insulin resistance) and hypertension significantly increase risk of DEATH AND COMPLICATIONS with COVID-19. Since there are lifestyle interventions that can quickly and effectively mitigate these problems (diet, exercise, sleep, stress reduction….) now would seem like a good time to take our epidemics of obesity and diabetes in hand with aggressive lifestyle interventions to decrease the mortality rate of COVID-19 infection.
Such measures do not require expensive drugs or expensive drug trials, they simply require knowledge, guidelines and the will to implement change in our daily habits. Yet there has been little discussion about this in the media or on the part of public health officials.
Lets look at obesity in the US.
From 1999–2000 through 2017–2018, the age-adjusted prevalence of obesity increased from
30.5% to 42.4%, and the prevalence of severe obesity increased from 4.7% to 9.2%.
The most effective tool for addressing obesity and diabetes is a very low carbohydrate diet.
Effects of the Low Carbohydrate, High Fat Diet on Glycemic Control and Body Weight in Patients With Type 2 Diabetes: Experience From a Community-Based Cohort
This study was a done in a community-based program, not an academic practice setting. That is significant since it demonstrates feasibility outside of academic centers with standard community resources. The results of this study confirmed the results of many previous studies done in academic settings including better blood sugar control, reduction or elimination of diabetic medications, and significant weight loss.
“All patients following the LCHF diet who initially took insulin had either a reduction or discontinuation of this therapy by their healthcare provider when clinically indicated, compared with less than a quarter of those receiving usual care.“
In another study done in Italy, significant weight reduction (7 kg), waistline reduction (7 cm.), fat mass reduction (3.8%) and systolic blood pressure reduction (10.5 mmHg) were achieved in 3 months with a Very Low Carbohydrate diet.
Middle and Long-Term Impact of a Very Low-Carbohydrate Ketogenic Diet on Cardiometabolic Factors: A Multi-Center, Cross-Sectional, Clinical Study (https://pubmed.ncbi.nlm.nih.gov/25986079/
Nina Teicholz had an opinion piece published in the Wall Street Journal on May 30, discussing the USDA dietary guidelines that have largely ignored a massive body of evidence supporting a Very Low Carbohydrate Diet for obesity and diabetes. She cites many studies that have been ignored by the USDA dietary guidelines committee. Here is here opening statement.
“Americans with obesity, diabetes, heart disease and other diet-related diseases are about three times more likely to suffer worsened outcomes from Covid-19, including death. Had we flattened the still-rising curves of these conditions, it’s quite possible that our fight against the virus would today look very different.”
But think about that simple statement, THREE TIMES MORE LIKELY TO SUFFER WORSENED OUTCOMES FROM COVID-19. Yet these conditions are highly responsive to lifestyle interventions that not only mitigate obesity, insulin resistance and high blood pressure, but also enhance immune function.
More from Teicholz’s opinion piece:
“Other studies have found that dietary changes can rapidly and substantially improve cardiovascular risk factors, including conditions like hypertension that are major risk factors for worsened Covid-19 outcomes. A 2011 study in the journal Obesity on 300 clinic patients eating a very low-carbohydrate diet saw blood pressure quickly drop and remain low for years. And a 2014 trial on 148 subjects, funded by the National Institutes of Health, found a low-carb diet to be “more effective for weight loss and cardiovascular risk factor reduction” than a low-fat control diet at the end of the 1-year experiment.“
In a recent letter to the editor published in the journal METABOLISM, Dr. Casey Means points out:
A diagnosis of diabetes has been a key indicator of the severity of COVID-19, and in this regard, the virus has relentlessly highlighted our global Achilles heel of metabolic dysfunction, and points to a prime opportunity to fight back. That fight, however, is not going to be won with Clorox, Purell, masks, or anti-IL-6 drugs. The fight will only be won through a serious commitment to improving everyone’s foundational metabolic health, starting with the lowest hanging evidence-based fruit: dietary and lifestyle interventions.
In 2 pages the letter describes multiple benefits of better glucose control relative to COVID -19 infection and the immune system as well as reduction of factors that lead to cytokine storm (terminal event for many COVID-19 patients). The letter also discusses the benefit of reducing environmental toxins (discussed in previous posts about COVID-19 and other health problems) that would likely benefit COVID-19 patients.
Research published April 18th, 2020 found that patients exposed to highest amount of environmental nitrogen dioxide (NO2) had increased risk of death fromCOVID-19, and that long-term exposure to this pollutant may be one of the most important contributors to fatality by compounding lung inflammation [20].
Minimizing exposure to environmental pollutants may serve a role in quelling the underlying pro-inflammatory state that characterizes metabolic disease and COVID-19 associated cytokine storms.
Other environmental toxins, including persistent organic pollutants (POPs) found in air, water, and food generated from pesticides and industrial chemicals, are also strongly implicated in the pathogenesis of metabolic syndrome; promoting “clean living,” toxin-avoidant strategies for patients as simple as emphasizing organic foods, home air purification, and non-toxic home supplies could be considered, although the clinical utility of these measures in the acute setting is unknown [21].
In discussing the white elephant in the room he states:
What is starkly missing is the clear, simple, and strong recommendation for no added sugar or ultra-refined carbohydrates, both of which are known drivers of postprandial hyperglycemia and inflammation. As a medical community, we must not miss the opportunity to serve patients with straightforward, evidence-based nutritional and lifestyle strategies to assist in glycemic control.
I would encourage you to follow the link and read the 2 pages supported by multiple peer-reviewed references.
An ancestral (paleo) diet is also very effective for addressing insulin resistance, diabetes type 2 and obesity. Multiple studies have demonstrated this. Although an ancestral approach is typically low carb it is not typically ketogenic, but a ketogenic ancestral diet (high in non starchy vegetables to support the gut microbiome) can be implemented by restricting fruits to one serving of berries per day and limiting starchy vegetables.
Even without severe carbohydrate restriction, an ancestral anti-inflammatory diet will quickly address insulin resistance, type 2 diabetes, and obesity. In this insulin resistance was reversed in 10 days.
And another study:
And another study
And here is a slide from one of my lectures with references on how an ancestral diet modulates immunity.
Leptin resistance, insulin resistance and obesity travel together. Here is yet another study demonstrating the effectiveness of an ancestral diet.
If you have obesity, diabetes or pre-diabetes the Very Low Carbohydrate version of the anti-inflammatory diet linked above would be the fastest and most effective intervention you can immediately employ to reduce your risk of succumbing to COVID-19. (Of course wear an N-95, follow good hygiene with hand-washing frequently, and use a HEPA filter or Corsi-Rosenthal box in your home, office, and enclosed work spaces)
In the context of the COVID 19 pandemic I will close with the usual summary.
Exercise, especially out of doors in a green space, supports the immune system
Get some sunshine and make sure you have adequate Vitamin D levels. Supplement with Vitamin D3 to get your levels above 30 ng/ml, >40ng/ml arguably better.
Eliminate sugar-added foods and beverages from your diet. These increase inflammation, cause metabolic dysfunction, and suppress immunity.
Eliminate refined-inflammatory “vegetable oils” from your diet, instead eat healthy fat.
Clean up your home environment and minimize your family’s exposure to environmental toxins by following recommendations at EWG.org with regards to household products, personal care products, and organic foods. (https://www.ewg.org/)
Drink water filtered through a high quality system that eliminates most environmental toxins.
HEPA filters or the home-made version (Corsi-Rosenthal box) used in your home or workplace can reduce circulating viral load as discussed on this website.
If you are eligible for vaccination, consider protecting yourself and your neighbor with a few jabs. Age > 50 and/or risk factors (Diabetes, pre-diabetes, insulin resistance, hypertension, obesity, heart disease, COPD, asthma, cancer treatment, immune suppression) suggests benefit from a booster. Risk for complications of boosters in adolescents, especially males, without risk factors, may equal benefit. Previous infection with Covid can be considered as protective as a booster. Discuss risk vs benefits with your doctor.
THIS WEBSITE PROVIDES INFORMATION FOR EDUCATIONAL PURPOSES ONLY. CONSULT YOUR HEALTH CARE PROVIDER FOR MEDICAL ADVICE.
Eat clean, drink filtered water, love, laugh, exercise outdoors in a greenspace, get some morning sunlight, block the blue light before bed, engage in meaningful work, find a sense of purpose, spend time with those you love, AND sleep well tonight.
The most comprehensive study on the use of these 2 drugs, including 96,032 patients in multiple hospitals and multiple countries shows increased risk of death with either of these two drugs in patients hospitalized with COVID-19. This was a retrospective study but offers the most amount of data to date on the issue of clinical efficacy and risk. You can read the full article https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(20)31180-6/fulltext.
Treatment
Death rate
ventricular arrhythmia
No drug
9.30%
0.30%
Hydroxychloroquine
18%
6.10%
Hydroxychloroquine plus Macrolide
23.80%
8.10%
Chloroquine
16.40%
4.30%
Chloroquine plus Macrolide
22.20%
6.50%
Macrolide is an antibiotic like Zithromax. Differences between no drug and all drug treatment categories statistically significant.
This was not a randomized prospective controlled clinical trial. However the data were adjusted for:
age, sex, race or ethnicity, body-mass index, underlying cardiovascular disease and its risk factors, diabetes, underlying lung disease, smoking, immunosuppressed condition, and baseline disease severity.
So far it is the best information we have available.
There have been many physicians who have supported the use of these drugs without randomized controlled trials based on anecdotal reports in the medical literature. Given the desparate situation without a known effective drug that is understandable.
The authors note:
The absence of an effective treatment against severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection has led clinicians to redirect drugs that are known to be effective for other medical conditions to the treatment of COVID-19. Key among these repurposed therapeutic agents are the antimalarial drug chloroquine and its analogue hydroxychloroquine, which is used for the treatment of autoimmune diseases, such as systemic lupus erythematosus and rheumatoid arthritis.
However, the use of this class of drugs for COVID-19 is based on a small number of anecdotal experiences that have shown variable responses in uncontrolled observational analyses, and small, open-label, randomised trials that have largely been inconclusive.
The combination of hydroxychloroquine with a second-generation macrolide, such as azithromycin (or clarithromycin), has also been advocated, despite limited evidence for its effectiveness.
This study is an important milestone, disappointing but illustrative of a common phenomenon in medicine.
Previous warnings about potential lethal heart rhythm issues were viewed with skepticism by armchair pundits claiming that there was not much data on sudden death related to use of these widely used drugs. Those pundits failed to understand that sudden death caused by prolonged QT interval (effect of these and many other drugs) cannot be diagnosed without an EKG during the event. When this occurs outside the hospital setting, or even in the hospital without a continuous EKG monitor on the patient, it goes unrecognized.
An important dictum in medicine is “first do no harm” (primum non nocere).
In the meantime, we do know what reduces risk:
Test/Trace/Isolate, social distance, MASKS4ALL, wash hands frequently, disinfect surfaces, show consideration for others. To understand why and how these measures can make a big difference you can go to this website. https://www.erinbromage.com/
Eliminate sugar-added foods and beverages from your diet. These increase inflammation, cause metabolic dysfunction, and suppress immunity.
THIS WEBSITE PROVIDES INFORMATION FOR EDUCATIONAL PURPOSES ONLY. CONSULT YOUR HEALTH CARE PROVIDER FOR MEDICAL ADVICE.
Eat clean, drink filtered water, love, laugh, exercise outdoors in a greenspace, get some morning sunlight, block the blue light before bed, engage in meaningful work, find a sense of purpose, spend time with those you love, AND sleep well tonight.
Sweden was a source of controversy for the choice against instituting a stay-home policy. As you compare Sweden with other Scandinavian countries above you will see a dramatic difference in deaths per million (cumulative), running 7 day average deaths per million per day, and doubling time. The higher the doubling time (in days) the more a country has slowed the spread. New Zealand is the obvious winner. Early and aggressive action, effective test/trace/isolate, excellent leadership and example by the president are the hallmarks of success in New Zealand. Of course New Zealand is a small island with minimal international business and tourism so the comparison is not fair. HOWEVER, their success and strategy are obvious.
The US failed (and continues to fail) on test/trace/isolate despite the bluster and misrepresentations from the Whitehouse. California and Washington instituted early measures with respect to stay-home but without adequate test kits all of US states have been unable to execute the test/trace/isolate strategy proven effective in other countries. President Trump promised California 100,000 nasal swabs per week three weeks ago. They have not arrived. (California Department of Public Health)
Thus comparing USA to Sweden we see that with adequate social distancing, test/trace/isolate, Sweden did almost as well (or as poorly) as the US where stay at home was employed on a variable time line and to different degrees between the states.
You can review worldwide data, download spreadsheets, choose countries for comparison here.
Test/Trace/Isolate + Social distance + Masks4all + cooperation = SUCCESS
Had the US responded early and effectively, stay-home could have ended very quickly and safely with much less economic disruption.
Poor Management = inadequate Test/Trace/Isolate and other measures.
The New England Journal of Medicine published an article discussing the failure of the
USA relative to Test/Trace/Isolate.
Eliminate sugar-added foods and beverages from your diet. These increase inflammation, cause metabolic dysfunction, and suppress immunity.
THIS WEBSITE PROVIDES INFORMATION FOR EDUCATIONAL PURPOSES ONLY. CONSULT YOUR HEALTH CARE PROVIDER FOR MEDICAL ADVICE.
Eat clean, drink filtered water, love, laugh, exercise outdoors in a greenspace, get some morning sunlight, block the blue light before bed, engage in meaningful work, find a sense of purpose, spend time with those you love, AND sleep well tonight.
New study (in mice) shows fast food makes the immune system more aggressive in a detrimental way.
Major points:
The immune system reacts similarly to a high sugar, high (unhealthy) fat and high calorie diet as to a bacterial infection.
Unhealthy food seems to make the body’s defenses (innate immune system) more aggressive in the long term. Even long after switching to a healthy diet, inflammation towards innate immune stimulation is more pronounced.
These changes may be involved in the development of arteriosclerosis and diabetes.
These changes are due to alterations in gene transcription (up-regulation of genes associated with inflammation)
This up regulation of pro-inflammatory genes persists even after converting to a healthier diet.
This study is an example of epigenetics, where an environmental factor (diet) alters the expression of genes. We know that regular consumption of a variety of colorful vegetables mediates many beneficial effects and part of that process involves altering the transcription of many genes related to health and our ability to defend against Oxidative Stress .
The epigenetic effect of nutrition can be transmitted to the next generation.
The epigenetic effects of diet include many aspects of health including cancer risk.
So avoid fast food and other forms of processed-refined foods. Eat a whole foods-ancestral diet that includes a variety of organic colorful vegetables and fruits, grass fed/finished meats and wild seafood. This will not only provide important micro and macro nutrients but will also turn up and turn on genes that prevent disease.
I have discussed the dangers of GMO foods and Roundup before.
The evidence continues to mount.
“A peer-reviewed article, published November 7, 2017, in the International Journal of Human Nutrition and Functional Medicine, demonstrates that GMOs are likely taking a heavy toll on our health. And a survey of 3,256 people who avoided them reported astonishing improvements in 28 health conditions.”
You can find a summary of the salient points from this scientific article here.
But I suggest you read the first few pages of the full article here.
The first few pages of this article describe the history of GMOs and how the warnings of FDA scientists were silenced by regulatory executives who were shills for the likes of Monsanto and other dangerous players in this sad history.
11 genetically modified food crops are currently grown for commercial consumption. The six major crops are soy, corn, cotton, canola, sugar beets and alfalfa which are used to feed humans and animals. Cottonseed and canola are also processed into “food-grade” oils and sugar beets are refined to make sugar.
All six major GMOs are engineered to be herbicide tolerant, to survive spray of weed killer (such as Roundup)
89% of GMOs grown in the US are herbicide tolerant
The most common herbicide involved is Roundup
94% of soybeans grown in the US are Roundup Resistant (RR)
Some varieties of corn and cotton have genes inserted that produce a toxic insecticide called Bt toxin.
76% of corn grown in the US is both Bt-producing and herbicide tolerant, 80% of cotton are both Bt and herbicide tolerant.
Roundup is not only used to kill weeds, but it is now sprayed heavily on crops immediately before harvest as a desiccant (drying agent) and large measurable amounts are found in the foods that you purchase in the supermarket.
In 1998 the FDA was sued by the Alliance for Bio-integrity and forced to turn over tens of thousands of pages of internal memos related to GMOs. FDA scientists repeatedly warned their superiors that GMO foods could create serious health risks such as allergies, toxins, antibiotic resistant diseases and nutritional problems. Michael Taylor, the former outside attorney for Monsanto and subsequent vice president of government and regulatory affairs for Monsanto was the political appointee in the FDA charged with overseeing GMOs!
On May 8, 2009,, the American Academy of Environmental Medicine published their policy paper on GMOs citing animal studies that revealed:
infertility,
immune dysregulation,
accelerated aging,
dysregulation of genes associated with cholesterol synthesis,
faulty insulin regulation, cell signaling and protein formation,
changes in the liver, kidney, spleen and gastrointestinal system
The AAEM recommended that the US government implement a moratorium on all GM foods and urged physicians to prescribe non-GMO diets.
But Monsanto prevailed and FDA officials ignored the warnings of their own scientists.
The three general categories of GMO danger include:
consequences of the GMO transformation process
the Bt toxin found in GMO corn and cotton
the herbicides-particularly Roundup, that are sprayed on most GMO foods and consumed by those who eat GMO food.
A study of Monsanto’s RR corn revealed 117 proteins and 91 small molecule biochemicals significantly different from natural corn. Some of those differences “enhance the effects of histamine, thus heightening allergic reactions” and two of the polyamines in the GMO corn have been implicated in the formation of carcinogens (nitrosamines).
The GMO process can produce a host of unintended changes in RNA, DNA, proteins and genes. And these changes can migrate and hybridize with non-GMO foods when the wind blows seeds from GMO plants into fields planted with non-GMO plants.
Altered Genes (transgenes) from GMO foods may “horizontally transfer” to humans or other organisms including the gut bacteria in humans that control much of our physiology.
Studies of rats fed GMO potatoes demonstrated adverse effects on every organ in young rats. Most changes occurred within 10 days. Disruption of organ growth, immune suppression and damage to organs of the immune system, thickening of the stomach and intestinal lining were noted.
Monsanto’s own data show that GM soybeans contain up to seven times the level of a natural allergen (trypsin inhibitor which also impairs protein digestion) and a doubling of soy lectin which impairs nutrient absorption. These were unintended consequences of the GMO process.
Monsanto’s MON810 Bt corn has 43 genes significantly altered in levels of expression. One of these genes which is normally switched off in non-GMO corn is switched on in the GMO version and it produces an allergenic protein.
Glyphosate is the major antibiotic in Roundup (yes Roundup is classified as an antibiotic). I have discussed the great hazards of glyphosate before. On October 24, 2017 JAMA published a study of the increase in measurable levels of glyphosate in humans.
The researchers compared urine excretion levels of glyphosate and aminomethylphosphonic acid (AMPA) in 100 people living in a Southern California community who provided samples during five clinic visits that took place between 1993 to 1996 and 2014 to 2016.
“What we saw was that prior to the introduction of genetically modified foods, very few people had detectable levels of glyphosate,” . “As of 2016, 70 percent of the study cohort had detectable levels.”
In July 2017, glyphosate was listed as a carcinogen by California.
A 2014 review concluded that:
Evidence is mounting that glyphosate interferes with many metabolic processes in plants and animals and glyphosate residues have been detected in both. Glyphosate disrupts the endocrine system and the balance of gut bacteria, it damages DNA and is a driver of mutations that lead to cancer.
There are many reasons to follow an organic, GMO-free, whole foods ancestral diet. Contamination with Roundup presents yet another compelling reason to choose your food wisely.
Some folks prefer videos to research articles, so below you will find both.
Here are a few links that will take you to articles related to this topic and quoted above.