- Exercise (aerobic and resistance training, in the gym, on the dance floor, outside in a greenspace, with friends and family)
- Get adequate restorative sleep (follow regular sleep habits, see also #s1, 3, 4 to 12)
- Enhance circadian rhythm (outdoor light exposure early in the day, avoid screen time prior to bed and/or use blue light blocking glasses and screen software, see also #1, #2, # 4 to 12)
- Reduce stress (meditation, yoga, tai chi, family time, #s1-3, 5-12)
- Engage in meaningful work
- Spend time with those you love
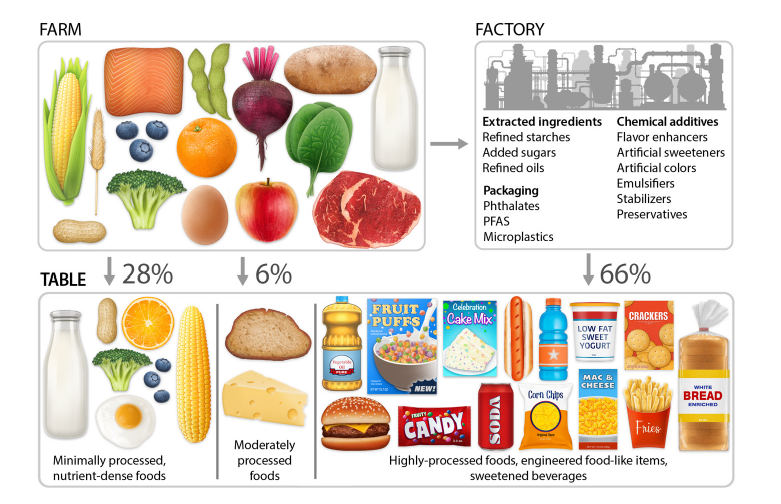
- Eat an anti-inflammatory (paleo) diet
- If overweight, employ therapeutic carbohydrate restriction (if on medications for diabetes this must be done under medical supervision following established published guidelines for medication adjustments)
- Spend time outdoors in a greenspace, especially early in the day. (Forest bathing)
- When working (on the computer) or reading indoors, do it in front of a large window to increase outdoor light exposure.
- Regularly use a sauna
- Consider brief cold immersion sessions (2-4 minutes of cold shower or cold-water immersion, approach this gradually)
Exercise: per minute spent, resistance training offers the most benefit. Second to resistance training is HIIT (High Intensity Interval Training) per unit of time spent. Finally moderate aerobic exercise (heart rate 60 to 80% of maximum predicted heart rate for age) places third for benefit per unit time spent. Most importantly, find some exercise that you enjoy and will sustain. Dancing, especially for seniors, combines the benefits of socialization, exercise, and simultaneous use of multiple brain areas, preserving and enhancing cognitive function in addition to mitigation of insulin resistance, chronic inflammation and cardiovascular risk. Engaging in sports that require coordination, balance, strength and complex movements also utilizes multiple areas of the brain simultaneously, providing for cognitive, metabolic and cardiovascular benefit. A single bout of exercise can increase insulin sensitivity for at least 16 h post exercise in healthy as well as diabetic subjects.
Sleep and Circadian Rhythm
Just one night of short-sleep causes acute insulin resistance. Chronic sleep deprivation contributes to chronic inflammation and insulin resistance. Go the bed and wake up on a consistent schedule. Avoid food and screen time for 3 hours before bed. Allow yourself at least 8 hours per night of sleep opportunity. Find relaxing routines to follow for an hour or two before bedtime. Avoid strenuous exercise in the evening. No caffeine after 12 noon. Getting outdoor light exposure early in the day facilitates restorative sleep. During sleep our brains flush out metabolic debris that accumulates during the day through the glymphatic system. Melatonin production during sleep provides multiple benefits including anti-inflammatory effects. Sleep in a cool very dark bedroom.
Optimizing sleep and circadian rhythm involves a combination of timing, environmental control, and biological signaling. These habits aim to align your internal master clock (the suprachiasmatic nucleus) with the external 24-hour light-dark cycle.
Summary Table: Daily Habits
| Habit | Timing | Primary Benefit |
| View Sunlight | First 60 mins of day | Sets the circadian “timer” |
| Exercise | Morning or Afternoon | Increases sleep pressure/adenosine |
| Last Meal | 3 hours before bed | Prevents metabolic circadian shift |
| Cool Room | All night | Facilitates core temp drop |
| Darkness | 1–2 hours before bed | Allows natural melatonin rise |
In my next posts I will explore items 5 through 12 above.
Yan R, Chen L, Lin G, Shi Y, Huang W, Mai Y, Sun J, Li D. Comparative effectiveness of different exercise modality on glycaemic control and lipid profile for prediabetes: systematic review and network meta-analysis. Front Endocrinol (Lausanne). 2025 Jul 24;16:1518871. doi: 10.3389/fendo.2025.1518871. PMID: 40778279; PMCID: PMC12328182. https://pubmed.ncbi.nlm.nih.gov/40778279/
Zhang L, Cheng X, Yang Y, Li X, Yuan Y. Optimal dosage and modality of exercise on glycemic control in people with prediabetes: a systematic review and network meta-analysis. Front Endocrinol (Lausanne). 2025 Apr 28;16:1560676. doi: 10.3389/fendo.2025.1560676. PMID: 40357204; PMCID: PMC12066256. https://pubmed.ncbi.nlm.nih.gov/40357204/
Huang L, Fang Y, Tang L. Comparisons of different exercise interventions on glycemic control and insulin resistance in prediabetes: a network meta-analysis. BMC Endocr Disord. 2021 Sep 6;21(1):181. doi: 10.1186/s12902-021-00846-y. PMID: 34488728; PMCID: PMC8422751. https://pubmed.ncbi.nlm.nih.gov/34488728/
Amaravadi SK, Maiya GA, K V, Shastry BA. Effectiveness of structured exercise program on insulin resistance and quality of life in type 2 diabetes mellitus-A randomized controlled trial. PLoS One. 2024 May 21;19(5):e0302831. doi: 10.1371/journal.pone.0302831. PMID: 38771888; PMCID: PMC11108169. https://pubmed.ncbi.nlm.nih.gov/38771888/
Alghadir AH, Gabr SA, Iqbal A. The effects of supervised aerobic training on dyslipidaemia among diabetic older patients. BMC Endocr Disord. 2024 Oct 9;24(1):212. doi: 10.1186/s12902-024-01745-8. PMID: 39385223; PMCID: PMC11462724. https://pubmed.ncbi.nlm.nih.gov/39385223/
Abdelbasset WK. Resistance Exercise Versus Aerobic Exercise Combined with Metformin Therapy in the Treatment of type 2 Diabetes: A 12-Week Comparative Clinical Study. Endocr Metab Immune Disord Drug Targets. 2021;21(8):1531-1536. doi: 10.2174/1871530320999200918143227. PMID: 32957900. https://pubmed.ncbi.nlm.nih.gov/32957900/
Li J, Cheng W, Ma H. A Comparative Study of Health Efficacy Indicators in Subjects with T2DM Applying Power Cycling to 12 Weeks of Low-Volume High-Intensity Interval Training and Moderate-Intensity Continuous Training. J Diabetes Res. 2022 Jan 13;2022:9273830. doi: 10.1155/2022/9273830. PMID: 35071605; PMCID: PMC8776485. https://pubmed.ncbi.nlm.nih.gov/35071605/
Findikoglu G, Altinkapak A, Yaylali GF. Is isoenergetic high-intensity interval exercise superior to moderate-intensity continuous exercise for cardiometabolic risk factors in individuals with type 2 diabetes mellitus? A single-blinded randomized controlled study. Eur J Sport Sci. 2023 Oct;23(10):2086-2097. doi: https://pubmed.ncbi.nlm.nih.gov/36622777/
Cox ER, Gajanand T, Keating SE, Hordern MD, Burton NW, Green DJ, Ramos JS, Ramos MV, Fassett RG, Cox SV, Coombes JS, Bailey TG. Effect of low-volume combined aerobic and resistance high-intensity interval training on vascular health in people with type 2 diabetes: a randomised controlled trial. Eur J Appl Physiol. 2024 Sep;124(9):2819-2833. doi: 10.1007/s00421-024-05473-8. Epub 2024 May 2. PMID: 38695912; PMCID: PMC11365856. https://pubmed.ncbi.nlm.nih.gov/38695912/
Li Z, Luo S, Bai X, Huang L, Guo H, Chen S, Wang D. Effects of different exercise types on vascular endothelial function in individuals with abnormal glycaemic control: a systematic review and network meta-analysis. PeerJ. 2025 Aug 8;13:e19839. doi: 10.7717/peerj.19839. PMID: 40792010; PMCID: PMC12338059. https://pubmed.ncbi.nlm.nih.gov/40792010/
Borghouts LB, Keizer HA. Exercise and insulin sensitivity: a review. Int J Sports Med. 2000 Jan;21(1):1-12. doi: 10.1055/s-2000-8847. PMID: 10683091. https://pubmed.ncbi.nlm.nih.gov/10683091/
Wojtaszewski JF, Richter EA. Effects of acute exercise and training on insulin action and sensitivity: focus on molecular mechanisms in muscle. Essays Biochem. 2006;42:31-46. doi: 10.1042/bse0420031. PMID: 17144878. https://pubmed.ncbi.nlm.nih.gov/17144878/
Böhm A, Weigert C, Staiger H, Häring HU. Exercise and diabetes: relevance and causes for response variability. Endocrine. 2016 Mar;51(3):390-401. doi: 10.1007/s12020-015-0792-6. Epub 2015 Dec 7. PMID: 26643313; PMCID: PMC4762932. https://pubmed.ncbi.nlm.nih.gov/26643313/
Reutrakul S, Van Cauter E. Sleep influences on obesity, insulin resistance, and risk of type 2 diabetes. Metabolism. 2018 Jul;84:56-66. doi: 10.1016/j.metabol.2018.02.010. Epub 2018 Mar 3. PMID: 29510179. https://pubmed.ncbi.nlm.nih.gov/29510179/
Antza C, Kostopoulos G, Mostafa S, Nirantharakumar K, Tahrani A. The links between sleep duration, obesity and type 2 diabetes mellitus. J Endocrinol. 2021 Dec 13;252(2):125-141. doi: 10.1530/JOE-21-0155. PMID: 34779405; PMCID: PMC8679843. https://pubmed.ncbi.nlm.nih.gov/34779405/
Koren D, Taveras EM. Association of sleep disturbances with obesity, insulin resistance and the metabolic syndrome. Metabolism. 2018 Jul;84:67-75. doi: 10.1016/j.metabol.2018.04.001. Epub 2018 Apr 6. PMID: 29630921. https://pubmed.ncbi.nlm.nih.gov/29630921/
Duffy, J. F., & Czeisler, C. A. (2009). Effect of Light on Human Circadian Physiology. Sleep Medicine Clinics. https://pubmed.ncbi.nlm.nih.gov/20161220/
Okamoto-Mizuno, K., & Mizuno, K. (2012). Effects of thermal environment on sleep and circadian rhythm. Journal of Physiological Anthropology. https://pubmed.ncbi.nlm.nih.gov/22738673/
Roenneberg, T., et al. (2012). Social Jetlag and Obesity. Current Biology. https://pubmed.ncbi.nlm.nih.gov/22578422/
Drake, C., et al. (2013). Caffeine effects on sleep taken 0, 3, or 6 hours before going to bed. Journal of Clinical Sleep Medicine. https://pubmed.ncbi.nlm.nih.gov/24235903/
Gooley, J. J., et al. (2011). Exposure to Room Light before Bedtime Suppresses Melatonin Onset and Shortens Melatonin Duration in Humans. The Journal of Clinical Endocrinology & Metabolism. https://pubmed.ncbi.nlm.nih.gov/21193540/
Speksnijder EM, Bisschop PH, Siegelaar SE, Stenvers DJ, Kalsbeek A. Circadian desynchrony and glucose metabolism. J Pineal Res. 2024 May;76(4):e12956. doi: 10.1111/jpi.12956. PMID: 38695262. https://pubmed.ncbi.nlm.nih.gov/38695262/
Engin A. Misalignment of Circadian Rhythms in Diet-Induced Obesity. Adv Exp Med Biol. 2024;1460:27-71. doi: 10.1007/978-3-031-63657-8_2. PMID: 39287848. https://pubmed.ncbi.nlm.nih.gov/39287848/
Koh JYJ, Tan CYH, Li M, Liu MH, Chew HSJ. The Effectiveness of Time-Restricted Eating as an Intermittent Fasting Approach on Shift Workers’ Glucose Metabolism: A Systematic Review and Meta-Analysis. Nutrients. 2025 May 15;17(10):1689. doi: 10.3390/nu17101689. PMID: 40431429; PMCID: PMC12114545. https://pubmed.ncbi.nlm.nih.gov/40431429/
Wang A, Vreijling J, Jongejan A, Rumanova VS, Versteeg RI, Kalsbeek A, Serlie MJ, la Fleur SE, Bisschop PH, Baas F, Stenvers DJ. The Acute Effects of Morning Bright Light on the Human White Adipose Tissue Transcriptome: Exploratory Post Hoc Analysis. Clocks Sleep. 2025 Aug 27;7(3):45. doi: 10.3390/clockssleep7030045. PMID: 40981208; PMCID: PMC12452623. https://pubmed.ncbi.nlm.nih.gov/40981208/
THIS WEBSITE PROVIDES INFORMATION FOR EDUCATIONAL PURPOSES ONLY. CONSULT YOUR HEALTH CARE PROVIDER FOR MEDICAL ADVICE.
Eat clean, drink filtered water, love, laugh, exercise outdoors in a greenspace, get some morning sunlight, block the blue light before bed, engage in meaningful work, find a sense of purpose, spend time with those you love, AND sleep well tonight.
Doctor Bob