I just listened to an NSPR interview with Dr. Jacob Glanville, an immuno-engineer, who has developed anti-bodies against the COVID19 virus. Dr. Glanville was featured in a Netflix movie “PANDEMIC’ which ironically aired in late January, after news of the novel corona virus had caught the public’s attention.
HISTORY: Dr. Glanville attended a “BIOTHREATS MEETING” in Washington DC in January 2020. Dr. Fauci (NIH Director of Allergy and Infectious Diseases) gave a talk at the conference in which he stated that COVID19 was “NO LONGER CONTAINABLE” and NIH was commissioning bio-tech companies to develop treatments. (mind you this was January 2020, Fauci already perceived a serious health threat to the USA and the world)
Several larger companies were in line ahead of Glanville’s to obtain federal funding for this project. Because of the critical nature of the problem Glanville decided on the spot to discuss with his colleagues at Distributed Bio an effort to develop antibodies against COVID 19 without funding. His company assigned researchers to work at night and on weekends to develop “high affinity” antibodies against COVID19. They used “superhuman”, a process and tool developed by his company, to access a “library” in a test tube with 76 billion human antibodies.
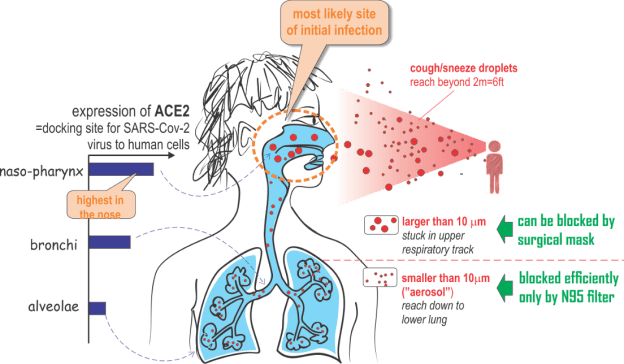
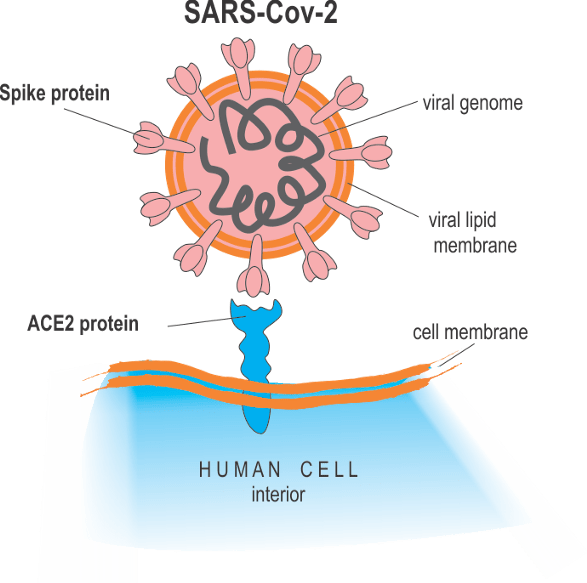
Following the SARS virus pandemic in 2003, the public domain had 5 “high affinity” antibodies against SARS. Because SARS and COVID19 are similar (both viruses enter human cells through the ACE2 receptor protein, both are forms of corona virus and can cause respiratory distress syndrome) , they took the 5 known SARS antibodies and “evolved” each one to work against COVID19. The weekend after Governor Newsome ordered a statewide shelter-at-home strategy in California, Dr. Glanville’s volunteer researchers made the breakthrough (working day and night). They found that the “evolved” antibodies from each of the 5 SARS antibodies offered high-affinity for the COVID19 virus. Each one of the five had been a success.
We took a series of five antibodies from around 2002 that were able to neutralize SARS. We were able to use technology in our laboratories to evolve those antibodies against SARS to adapt them to recognize COVID-19.
We tried with five different antibodies because we weren’t sure which one would work the best. All five worked so we have a pretty powerful tool chest available to us right now to produce a final therapeutic.
From the interview:
What is the next step?
We are sending [the antibodies] to the military for confirmation testing and to Charles River Laboratories for safety and tox characterization. We’ve partnered with two different companies that will help us scale up large batches of the antibody for production. We’re in discussions to start human phase one/two trials that would happen at the end of the summer.
The earliest this could possibly reach clinical application would be September 2020 under the compassionate use act if everything goes smoothly and efficiently and red-tape is overcome.
The story of this rapid response by volunteers working after hours and on weekends, long before the Whitehouse started taking action, represents a remarkable effort undertaken by a private company with no public funding. Many hurdles must be overcome to bring this bio-therapeutic to patients. Once this becomes available it offers great hope for an effective treatment.
THIS WEBSITE PROVIDES INFORMATION FOR EDUCATIONAL PURPOSES ONLY. CONSULT YOUR HEALTH CARE PROVIDER FOR MEDICAL ADVICE.
Eat clean, drink filtered water, love, laugh, exercise outdoors in a greenspace, get some morning sunlight, block the blue light before bed, engage in meaningful work, find a sense of purpose, spend time with those you love, AND sleep well tonight.
Doctor Bob