Preliminary (not yet peer reviewed) data on mortality rates with COVID-19 infection from Indonesia show a dramatic increase in death rates associated with low vitamin D status.
| Relative Risk of DEATH Corrected for age, sex, and co-morbidities |
Vitamin D level (ng/ml)
|
| 10.1 | <20 |
| 7.6 |
21-29
|
| 1
|
>= 30 |
Prabowo, Patterns of COVID 19 Mortality and Vitamin D, Indonesian Study, Ap 26, 2020 BMJ
This study was a retrospective cohort study of 780 cases of laboratory confirmed COVID-19 in Indonesia. Age, sex, co-morbidity (hypertension, diabetes, obesity etc.) and Vitamin D levels were extracted from medical records. The differences between patients with various levels of vitamin D were statistically significant and CLINICALLY SIGNIFICANT.
If there were a drug that reduced mortality by 10 fold it would be a best-seller/blockbuster drug.
“When controlling for age, sex, and comorbidity, Vitamin D status is strongly associated with COVID-19 mortality outcome of cases.”
Association does not equal causation but this profound degree of association warrants further consideration. Is it possible that Vitamin D insufficiency could cause such a profound influence on death rates with a viral infection?
Before we answer that question let’s look at some other data. Risk of death with COVID-19 dramatically changes with latitude (sunlight exposure reflecting Vitamin D making capability):
| Latitudes | Hospitalizations COVID-19 | Deaths COVID-19 |
| Northern | 22% | 5.2% |
| Equator | 9.5% | 3.1% |
| Southern | 8.7% | 0.7% |
You can read about this data here.
The authors state:
“Although it is more likely that any protective effect of vitamin D against
Covid19 is related to suppression of cytokine response and reduced severity/risk for ARDS, there is also evidence from a meta-analysis that regular oral vitamin D2/D3 intake (in doses up to 2000 IU/d without additional bolus), is safe and protective against acute respiratory tract infection, especially in subjects with vitamin D deficiency. It therefore seems plausible that Vitamin D prophylaxis (without over-dosing) may contribute to reducing the severity of illness caused by SARS-CoV-2, particularly in settings where hypovitaminosis D is frequent. This will include people currently living in Northern countries and those with underlying gastroenterological conditions where vitamin D deficiency is more prevalent. This may become even more important with absence of sunlight exposure as a consequence of “shut-down” measures to control the spread of Covid19. For this to be effectively implemented will require worldwide government guidelines, and further studies looking at possible impacts of vitamin D deficiency on Covid-19 outcomes are urgently needed.”
Plenty of references are provided for their discussion so I encourage you to not only read the publication but further explore their references.
The importance of Vitamin D for proper immune function has been well studied and known for a long time.
“Vitamin D metabolizing enzymes and vitamin D receptors are present in many cell types including various immune cells such as antigen-presenting-cells, T cells, B cells and monocytes. In vitro data show that, in addition to modulating innate immune cells, vitamin D also promotes a more tolerogenic immunological status. In vivo data from animals and from human vitamin D supplementation studies have shown beneficial effects of vitamin D on immune function, in particular in the context of autoimmunity”
“Especially in the field of human immunology, the extra-renal synthesis of the active metabolite calcitriol—1,25(OH)2D—by immune cells and peripheral tissues has been proposed to have immunomodulatory properties similar to locally active cytokines”
Now consider this startling fact. At the turn of the century (2001-2004) 70% of the US population over age 12 had 25 Hydroxy-Vitamin D levels LESS THAN 30 ng/ml.
And the situation has not improved since that study. In the chart above that places 70% of the US population in the groups with 7.6 to 10.1 times increased risk of death from COVID 19 compared with those having “normal” levels (>30 ng/ml).
Conclusions
“National data demonstrate a marked decrease in serum 25(OH)D levels from the 1988–1994 to the 2001–2004 NHANES data collections. Racial/ethnic differences have persisted and may have important implications for known health disparities. Current recommendations for vitamin D supplementation are inadequate to address the growing epidemic of vitamin D insufficiency.”
Multiple studies on COVID-19 have shown higher mortality rates amongst blacks. Although this is likely related to many socio-economic and nutritional factors, blacks have consistently shown significantly lower Vitamin D levels in the US compared with other ethnic/racial groups.
During the 2009 Viral Pandemic, death rates were observed to increase with distance from the equator, similar to the COVID-19 observations.
Death rates from COVID-19 in ITALY, where Vitamin D status is much lower compared to the rest of Europe, have been higher than other countries in Europe.
And a large report on Vitamin D status in Europe and the Middle East states:
“A low vitamin D status was also associated with increased mortality risks as extensively reviewed” with references (3, 27, 206, 209).
A brilliant video podcast on the relationship between Vitamin D and COVID-19 can be viewed here.
And if you wish to further explore the health effects of Vitamin D you can watch this:
Insufficient Vitamin D levels are associated with almost every risk factor for Morbidity and Mortality with COVID-19 including Diabetes, Insulin Resistance, Obesity, Hypertension and Cardiovascular Disease.
Many of the concerns covered in Ivor Cummin’s podcast above have been covered in previous posts here including the importance of Vitamin K2 and other fat soluble vitamins, the importance of SUNSHINE for general health and immune function, and the importance of a nutrient dense whole food diet rich in wild seafood and grass fed animal sources of protein. Almost every cell in the body has receptors for Vitamin D. The most beneficial sources of Vitamin D include sunshine and food sources. Supplementation is often necessary to achieve levels above 30 ng/ml, especially during the winter months (when respiratory viruses strike) and increase with distance from the equator.
The deleterious effects of inadequate Vitamin D cannot be overstated. The consequences below only address the effects of Vitamin D insufficiency on bone health but the causes and prevention are important to understand. Vitamin D deficiency = Immune Deficiency and is likely strongly and causally related to increased risk of death with COVID-19.
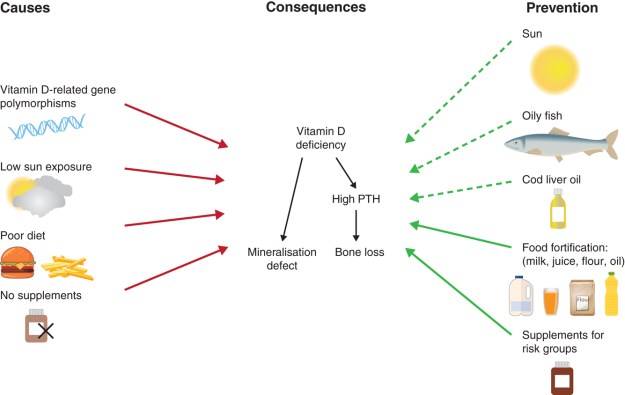
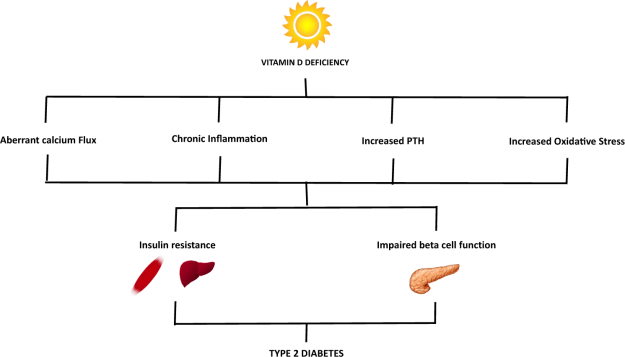
Here is an image that links Vitamin D deficiency to Diabetes, inflammation and oxidative stress:
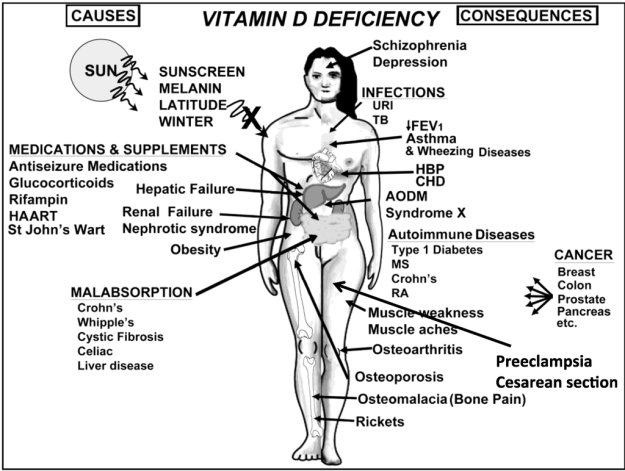
And here is a good description of the consequences of inadequate Vitamin D.
So what do you think? Is it possible that Vitamin D insufficiency could cause such a profound influence on death rates with a viral infection? Lets look a little closer.
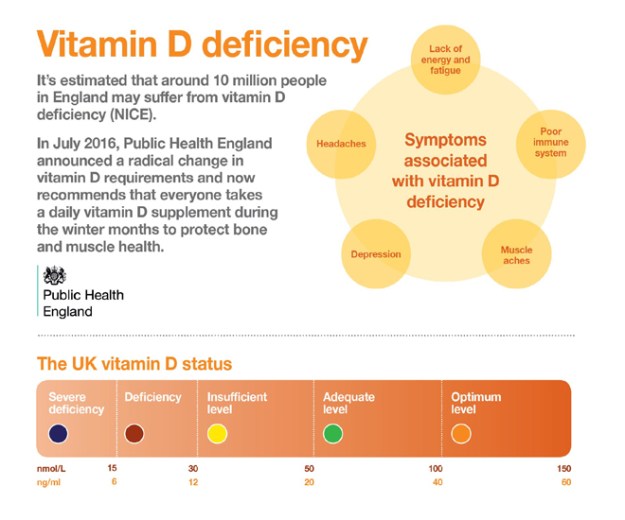
The Public Health system in UK has been concerned about Vitamin D deficiency:
And once again here is how inadequate Vitamin D interacts with the co-morbidities that are unequivocally associated with increased death rates associated with COVID-19 infection.
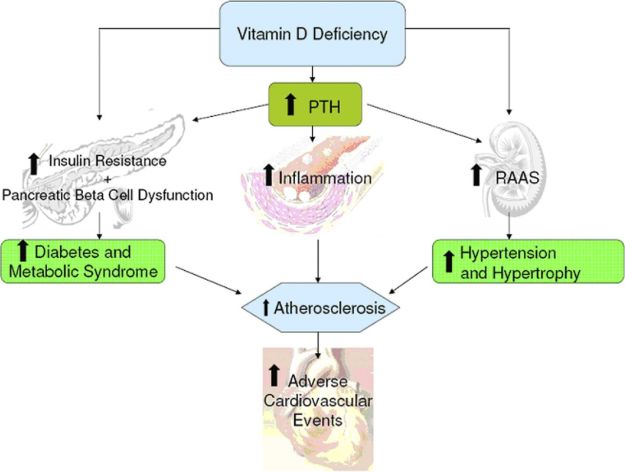
PTH is parathyroid hormone. The RAAS above refers to the renin-angiotensin system hypertension effects mediated through the kidney. The chronic inflammation associated with inadequate Vitamin D leads to atherosclerosis and cardiovascular events, diabetes, insulin resistance, metabolic syndrome which all have positive feedback effects on each other. They all increase risk of death with COVID-19.
Again I ask, what do you think? Is it possible that Vitamin D insufficiency could cause such a profound influence on death rates with a viral infection?

(The thing speaks for itself)
RX from the doctor could read:
Sunbath for 15 minutes daily between 1100 AM and 1 PM (wear a hat, sunglasses, bathing suit optional depending on circumstances and privacy)
Eat fatty fish frequently.
Get your 25 hydroxy-vitamin D levels checked, if < 30 ng/ml increase the above.
Supplement in the winter.
Further reading can be found here:
Vitamin D Insufficiency is Prevalent in Severe COVID-19
Vitamin D Supplementation Could Possibly Improve Clinical Outcomes of Patients Infected with Coronavirus-2019 (COVID-2019)
Latitude Dependence of the COVID-19 Mortality Rate—A Possible Relationship to Vitamin D Deficiency?
Vitamin D supplementation could prevent and treat influenza, coronavirus, and pneumonia infections
low population mortality from COVID‐19 in countries south of latitude 35 degrees North–supports vitamin D as a factor determining severity
Covid‐19, and vitamin D
THIS WEBSITE PROVIDES INFORMATION FOR EDUCATIONAL PURPOSES ONLY. CONSULT YOUR HEALTH CARE PROVIDER FOR MEDICAL ADVICE.
Eat clean, drink filtered water, love, laugh, exercise outdoors in a greenspace, get some morning sunlight, block the blue light before bed, engage in meaningful work, find a sense of purpose, spend time with those you love, AND sleep well tonight.
Doctor Bob

Thx Bob for the research on Vitamin D. Right after my dx with polycythemia I met with a clinical dietitian here in South Fla. One of the supplements she strongly encouraged to take was Vitamin D once daily at 5000 mg. I honestly believe it has kept me free from a lot of the seasonal viruses we have down here. The other interesting development for me is that my wife recently took a course on aromatherapy and learned quite a bit about the use of essential oils as an alternative treatment for many things. Ironically, since I began using the oils (lemongrass, frankincense, peppermint, lavender, etc) about 6 months ago I have not needed ANY phlebotomies to reduce my HCT level. Anyway, I appreciate the thoughtful advice on Vitamin D.
Stay healthy and safe from this awful COVID. Hope to maybe see you this summer in NJ if things ever return to “normal”.
Chris McClave
Prep 69er
Glad to hear it Chris. I think you meant 5000 iU for the Vitamin D, which is a good dose.
Pingback: Vitamin D for All, the time is right | Practical Evolutionary Health